

Translate this page into:
Prevalence and Determinants of Substance Abuse Among Slum Dwellers in Islamabad- Pakistan
✉Corresponding author email: drfaizabashir@yahoo.com
Abstract
Background:
In Pakistan, slums are illegal settlements that are always left out in health surveys. However, studies around the world show that substance or drug abuse is higher among slum dwellers and may have different patterns and determinants which need to be studied in order to frame targeted programs and policies. The present study was aimed at estimating the magnitude, as well as determinants of substance/drug abuse among slum dwellers in Islamabad, the capital city of Pakistan.
Methods:
A community-based cross-sectional study was conducted among the residents of slums/nomadic settlements of Islamabad. A population of 207 individuals was calculated as the appropriate sample size. Both female and male participants aged 15 years and above, from 9 randomly selected slum clusters in Islamabad provided their consent to participate in the study. From each cluster, 23 households were selected, and from each household one individual was randomly selected for estimating the prevalence of substance abuse. All those who were abusing substances were counted as cases and others as controls for case-control analysis. A structured questionnaire was used to gather information on demographics, trends, types of substances abused, risk factors for getting engaged in substance abuse, whether they had tried to quit at any stage, and what difficulties they faced when trying to quit. Results were entered and analyzed using Epi-info version 7.2.
Results:
A total of 204 participants were enrolled in this study. Among these, 68 (33.3%) were substance or drug abusers. Bivariate analysis of the risk factors indicated that easy access to drugs in slum areas (OR: 20.3, p= 0.000), exposure to tobacco smoking (OR: 8.8, p= 0.000), and being a working child (OR: 6.0, p= 0.000), were strong predictors of substance abuse. Education (OR: 0.2, p= 0.000), and living with own parents during childhood (OR: 0.7 p= 0.2) had protective effects against substance abuse.
Conclusion and Implications for Translation:
The study concluded that the following were the determinants of substance/drug abuse among the slum dwellers in the study: easy access to drugs, high rate of tobacco consumption, poverty, illiteracy, and being a working-child. Specific policies and plans focusing on law enforcement for curbing the illegal drug sales and reduction of child labor, along with the provision of education, should be devised and implemented to help these neglected communities and modify the identified determinants.
Keywords
Substance Abuse
Drug Abuse
Slum Dwellers
Case-control
Islamabad
Pakistan

Introduction
Substance abuse in Pakistan is one of the major causes of concern that affects almost all segments of society. In 2013, an estimated 6% (6.7 million adults) of the population in Pakistan were abusing drugs or substances.1
Substance abuse not only has devastating effects on the physical and psychological wellbeing of people, but also has adverse effects on the economic growth of the country. Particularly, heroin abuse is spreading at a high rate, especially among those between the ages of 15 and 39 years.1 Pakistan has extensively been exposed to illegal opium trafficking and abuse, with an emergence of methamphetamine use as of late. Cannabis usage appears to be most prevalent in people aged 30 to 34, whereas heroin use appears to be most prevalent in people aged 35 to 39.1
According to a study by Khalily2 on developing a coordinated response to drug abuse in Pakistan, the average age of initiation of drug use is 18 years and drugs are more prevalent among the lower and lower- middle classes of society in some areas of the country.2 Cannabis was found to be the most commonly used drug in Pakistan affecting 3.6% of the adult population. Opiates are used by almost 1% of overall drug users.3
The increasing point of concern is the high prevalence of non-medical use of prescription drugs nationwide, particularly among women. Among addicts, women have a higher prevalence of drug use when compared to men in Pakistan. A high proportion of women that have confirmed their drug use, revealed that they have resorted to misusing opioid-based painkillers, and to a lesser extent tranquilizers and sedatives, which are readily available in pharmacies.2 Alcohol, cocaine, hallucinogens, heroin, inhalants, ketamine, marijuana (cannabis/bang), methamphetamine (white crystalline powder), prescription opioids, prescription sedatives (tranquilizers, depressants) steroids (anabolic), tobacco, nicotine, niswar are reported substances that are abused.
The situation is of concern due to the high prevalence of Hepatitis B and C, which is associated to injection drug use. The number of people injecting drugs is estimated to be 4.3 million (0.4%) across the country.1 Factors responsible for the expanding drug use in Pakistan include the easy access to drugs at very low prices, unemployment, individual's dissatisfaction with their economic situation, low level of education, lack of education about drugs within the family and educational institutions, peer pressure, and negligence of parents.4,5
Pakistan is situated in the northwestern part of the south Asian subcontinent, comprising a total land area of 796,096 square kilometers. Administratively, Pakistan has four provinces named Punjab, Sindh, Khyber Pakhtunkhwa, and Baluchistan along with the Federally Administrative Tribal Areas (FATA), and the Gilgit Baltistan region.6 According to the 2017 census report, Pakistan has a total population of almost 207 million people.7 Pakistan is an agricultural country, that used to have more than 70% of the population living in rural areas, but during the last few decades, the country has faced rapid urbanization. The share of Pakistan's urban population was 28.3% in 1981, rising to 32.5% during 1998, and reaching to 37.9% during 2017.8 High urbanization trends arise mainly due to poor agricultural policies by the government, inadequate employment avenues, and low quality of life in rural areas.9
Rapid urbanization has generated some public health issues due to limited urban infrastructure and housing facilities in the country. People from lower socioeconomic classes are unable to build appropriate shelters in large cities, leading to the building of squatter housing settlements known as slums. According to Encyclopedia Britannica, a slum is defined as “a residential area that is physically and socially deteriorated and where satisfactory family life is impossible.”10 Poor housing is the main index of slum populations which includes poor dwellings, inadequate infrastructure, absence of family privacy, and no space for recreational facilities.11 In addition to these, illiteracy, unemployment, poverty, poor health, and deficient sanitation are the common features of the people living in these slums.11 In most cases, the government or any other health authorities do not usually account for the basic living requirements of slum dwellers.12
Though the living conditions, health facilities, and health services are not optimal for even the general population, they are far superior compared to those in the slums, due to access to better housing, employment opportunities, and health services. As the settlements are illegal and temporary, they are unable to become a focus for the facilitation of infrastructure, health and education facilities, and law regulation and enforcement. All these factors make the slum dwellers “underserved population” and thus vulnerable. The growing number of slum areas in Pakistan is a major issue exacerbated by the occurrence of floods, growing urbanization, the unplanned growth of cities, and the concentration of employment opportunities within urban settlements. Pakistan's slums have many similarities compared to other low- and middle-income countries (LMICs), such as overcrowding, lack of housing, inadequate hygiene, extremely poor sanitation, precarious economic situation, low education levels and limited to no access to healthcare. Also, there is no healthcare delivery system focused on these underserved populations. Literature shows that the slums are at the worst of conditions, especially concerning their healthcare. Slums are missed in health and other global surveys of Pakistan. However, studies around the world show that substance abuse is relatively high among slum dwellers, which may have different patterns that need to be studied so that information can be used to target programs and policies.13-15
Therefore, the purpose of this study was to provide an insight into the gravity of substance/drug abuse and identify its determinants among such vulnerable populations.
Methods
A community-based, cross-sectional study was performed, involving the populations living in slums/nomadic settlements of Islamabad. Adults from both sexes and aged 15 years old and above, were enrolled from selected clusters, and consented to participate in the study. Mentally unstable individuals, and those that could not comprehend the questions asked, were excluded from the study.
The survey was planned in a two-staged cluster sampling manner, to ensure adequate coverage. According to the latest list from Islamabad's (Federal Capital of Pakistan) Capital Development Authority (CDA), almost 18 settlements were present, with an estimated population of 80,000 people. A total of 9 out of the 18 settlements were randomly selected to cover approximately 50% of the area. Epi Info software16 (CDC Epi Info 2010) was used to calculate the sample size for the population-based survey, with a 95% confidence limit, a 5% margin of error, and a 5% substance abuse prevalence. Assuming a design effect of 2.00, the minimum sample size was 154 people; then, by adding a difference of 20% to account for the possible non-response rate, the sample size became 207 people. From each cluster, and in a randomized manner, a total of 23 households were selected. Subsequently, one individual from each household was randomly selected for estimating the prevalence of substance abuse. Substance abusers were considered case subjects, while non-substance abusers were deemed as control subjects.
The questionnaire contained both close- ended and open-ended questions on demographic characteristics, type and pattern of use of illicit drugs (alcohol, cocaine, hallucinogens, heroin, inhalants, ketamine, marijuana (cannabis/bang), methamphetamine (white crystalline powder), prescription opioids, prescription sedatives (tranquilizers, depressants) steroids (anabolic), tobacco use, nicotine, naswar, time of initiation, reason for continuing with this abuse, and efforts of quitting, if attempted at any time. The questionnaire was administered by a team of trained data collectors who use to have a prior meeting with the community head for permission to carry out the survey.
Ethical considerations
Ethical clearance was obtained from the Institutional Review Board (IRB) of the Pakistan Health Research Council (PHRC), which is the agency with the mandate to issue ethical clearances to in-country research studies. Informed written consent was obtained in Urdu (national language) from the respondents. There were a majority of uneducated members in the population, thus a community member accompanied the researchers while taking consent, who would explain the research study objectives and requirements to the respondents. Participants were assured of the confidentiality of the information by not using personal identifiers. They were also given the choice to leave the study at any point if they wanted to.
Results
Sociodemographic characteristics
A total of 204 participants were enrolled in the study. Among these, 68 (33.3%) were found to be drug users, and as such, were considered the case subjects; this would leave a total of 136 (66.7%) participants to be deemed as the control subjects. The majority of of participants were male, constituting a total of 187 participants (91.7%), while only 36 participants (8.3%) were female. The mean age of the respondents was 39.5+14 years (range 16-85 years), and the mean age of drug users was 35.3 ± 13.7 (range 17-41.5 years) (Table 1). The age wise distribution showed the highest prevalence of substance abuse in ages 30-44 years followed by ages 15-29 years. Drug use is less prevalent in older age groups. (Figure 1).
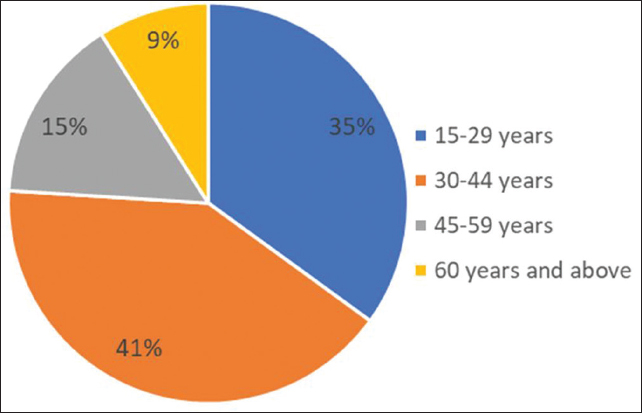
- Prevalance of drug abuse among different age groups in slum dwellers of Islamabad
| Demographic information | Frequency among cases (%) | Frequency among controls (%) |
|---|---|---|
| Age (years) | ||
| Mean age±standard deviation | 35.314 years (17-41.55 years) | 40±13 (16-85 years) |
| 15-29 years | 24 (35.29) | 24 (17.65) |
| 30-44 years | 28 (41.18) | 60 (44.12) |
| 45-59 years | 10 (14.71) | 36 (26.47) |
| 60 years and above | 6 (8.82) | 16 (11.76) |
| Educational level | ||
| Uneducated | 42 (62.00) | 72 (52.00) |
| Up to primary | 20 (29.00) | 48 (35.00) |
| Up to high school | 6 (9.00) | 12 (9.00) |
| College and above | 0 (0.00) | 2 (1.40) |
| Monthly income | ||
| ≤10,000 PKR* | 30 (44.00) | 38(28.00) |
| 10-20,000 PKR | 4 (4.80) | 80 (59.00) |
| 20-40,000 PKR | 34 (50.0) | 17 (12.00) |
| 40,000 and above | 0 (0.00) | 1 (0.70) |
| *154.34 PKR (Pakistan Rupees)=$1.00 (U.S. Dollar) | ||
Risk factors for substance/drug abuse
Drug abuse was reported by 33.3% (n= 68) of the respondents; 38% of these abusers were addicted to two or more types of drugs. A total of 84% of the drug users were working since their childhood, while 67% were trying to earn money to support their drug addiction. The majority (66%) of the substance abusers were also tobacco smokers. Easy access to illegal drugs was reported by 61% of the cases. Furthermore, of the case subjects, 48% were living with parents during their childhood, 32% never went to school, and 45% were exposed to substance abuse because their family member use drugs (Table 2).
| Risk factors | Percentage among cases (%) | Percentage among controls (%) |
|---|---|---|
| Never attended the school | 32.0 | 67.0 |
| Lived with parents during childhood | 48.0 | 57.0 |
| Use of drugs by family member | 45.0 | 27.2 |
| Easy access to drugs | 61.0 | 7.3 |
| Worked as a child | 84.0 | 46.3 |
| Smokers status | 66.0 | 18.0 |
Bivariate analysis of the risk factors indicated that easy availability of drugs in slum areas (OR: 20.3; p= 0.000), exposure to tobacco smoking (OR: 8.8; p= 0.000), being a working child (OR: 6.0; p= 0.000) and use of drugs by a family member (OR: 2.2; p= 0.005) were the strong predictors of high substance abuse among slum area residents. It was further determined that education (OR:0.2;p= 0.000) and living with parents during childhood (OR: 0.7; p= 0.2) had a protective effect against substance abuse (Table 3).
| Risk factors | Odds Ratios (OR) | 95% Confidence Interval | P- value |
|---|---|---|---|
| Easy access to drugs | 20.3 | 9.0-45.6 | 0.000 |
| Smokers status | 8.8 | 4.5-17.3 | 0.000 |
| Worked as a child | 6.0 | 2.8-12.4 | 0.000 |
| Use of drugs by family member | 2.2 | 1.2-4.1 | 0.005 |
| Never attended school | 0.2 | 0.1-0.4 | 0.000 |
| Lived with parents during childhood | 0.7 | 0.3-1.2 | 0.2 |
Discussion
The study found a high prevalence of substance abuse (33.3%) among dwellers in slum settlements in Islamabad. This is much higher when compared to the estimated country report in 2013.3 A higher than expected prevalence of substance abuse in special communities like slums are also reported in other studies across the globe; in India, for example, it is reported to be 43%.17-19 The present study observed that earlier exposure to tobacco smoking made a person more prone to indulge in illicit drug abuse which is strongly supported by the study by Ghulam et al.20
There are numerous factors influencing the engagement in substance abuse such as the influence of friends or peer pressure, social and family stresses, or someone else in the family using drugs.6,21 In addition, the study indicated that living with parents as a child had a protective effect against substance abuse. However, belonging to a broken family, living on your own, or living as a working child, were suggestive of being strong predictors of substance abuse. This was supported by a prior study, which described factors such as problems with parental or marital relations, a relationship breakup, the desire to escape stressful life events, or feelings of failure, as being contributors to substance abuse.22
Another important finding of the present study was that easy access to drugs was one of the strongest predictors of substance abuse within slums. Illegal and unregulated communities seem to be the hub of illicit activities and drugs, and where these are easily accessible, thus increasing the exposure to the population.22 Findings also showed the protective effect of education, which is largely supported by other studies, thereby further strengthening the argument that education has a special place while addressing such issues.17-22
Limitations
The study was a non-funded activity, therefore the lack of resources was a major limitation to going beyond a specified geographical location, namely Islamabad. Although the key characteristics of the slum areas remain the same, a study with limited geographical representation is a limitation and our results lack the element of generalizability for the slum areas of the entire Pakistan. However, this pilot study provided some insight to the gravity of the situation and warrants further large-scale interventional studies to adress the modifiable determinants of substance abuse.
Conclusions and Implications for Translation
The prevalence of substance abuse among Islamabad residents was alarming. The determinants of substance abuse included unregulated and illegal drug sales, high rate of tobacco consumption, poverty, illiteracy, social and family issues, and being a working child. Though these determinants are inherent to slum settlements, they are largely modifiable. It is recommended that the menace of substance abuse among such vulnerable populations require strategic interventions such as enacting laws for curbing the illegal drug and tobacco sales and their accessibility, regulating child labor practices, and the provision of health and behavior change education.
Compliance with Ethical Standards
Conflicts of interest:
All authors hereby declare that they have no conflict of interest that may have affected the results obtained in the study.
Financial Disclosure:
Nothing to declare.
Ethics Approval:
Ethical clearance was obtained from the Institutional Review Board (IRB) of Pakistan Health Research Council (PHRC. Informed written consent was obtained from respondents in Urdu (national language). Participants were assured of the confidentiality of the information by not using personal identifiers. They were also given a choice to leave the study at any point if they wanted to.
Disclaimer:
None.
Acknowledgments:
As this was a non-funded activity supported by Pakistan Health Research Council; the logistics and human resource was graciously provided for this research study and we extend our gratitude for this support to PHRC and its personnel.
Funding/Support:
The publication of this article was fully supported by the Global Health and Education Projects, Inc. (GHEP) through the Emerging Scholar's Grant Program (ESGP). The information, contents, and conclusions are those of the authors and should not be construed as the official position or policy of nor should any endorsements be inferred by ESGP or GHEP.
References
- Horrendous situation of substance abuse in Pakistan: a bird's eye view on socio-demographics. J Alcohol Drug Depend. 2015;3:201.
- [Google Scholar]
- Developing a coordinated response to drug abuse in Pakistan. J Interprof Care. 2010;24(2):168-172.
- [CrossRef] [Google Scholar]
- Drug Use in Pakistan 2013. Ministry of Interior and Narcotics Control Narcotics Control Division Government of Pakistan; Published 2014 (accessed )
- National Drug Abuse Assessment 2006/07. Ministry of Narcotics Control. Published 2007 (accessed )
- [Google Scholar]
- Demographic profile and etiological factors of starting drugs among patients with drug addiction. J Coll Physicians Surg Pak. 2011;21(2):125-6.
- [Google Scholar]
- 2013. Pakistan Demographic and Health Survey 2012-13. Islamabad, Pakistan and Calverton, Maryland, USA: NIPS and ICF International; (accessed )
- 2017. Pakistan Tehsil Wise for Web Census 2017. Pakistan Bureau of Statistics; Published 2017 (accessed )
- 2019. Pakistan Demographic and Health Profile 2017-2018. Islamabad, Pakistan and Rockville, Maryland, USA: NIPS and ICF; (accessed )
- Socio-economic status of transferred and non-transferred urban slums: a case study from Faisalabad. Pakistan Institute of Development Economics. (accessed )
- [Google Scholar]
- Britannica, The Editors of Encyclopedia. “Slum.” Encyclopedia Britannica. Published 2008 (accessed )
- [Google Scholar]
- Exploration of socio-economic problems of the inhabitants of slum areas and their impact on vicinity residents: a case study of Arifwala Pakistan. Sci Int. 2016;28(5):7-13. (Lahore)
- [Google Scholar]
- Child criminalization at slum areas in Dhaka City. American Journal of Psychology and Cognitive Science. 2015;1(4):107-111.
- [Google Scholar]
- A study of drugs and substance abuse among adolescents of slum dwellers. Int J Indian Psychol. 2016;3(3):58.
- [Google Scholar]
- Slum health: diseases of neglected populations. BMC Int Health Hum Rights. 2007;7(1):2.
- [CrossRef] [Google Scholar]
- Co-occurrence of behavioral risk factors of common non-communicable diseases among urban slum dwellers in Nairobi, Kenya. Glob Health Action. 2015;8:28697.
- [CrossRef] [Google Scholar]
- Version 7.2. Atlanta. GA: Centers for Disease Control and Prevention;
- Substance abuse amongst the street-children in Guwahati City, Assam. Ann Med Health Sci Res. 2014;4(3):233-241.
- [CrossRef] [Google Scholar]
- An epidemiological study on substance abuse among college students of north India. Int J Med Sci Public Health. 2013;2(3):562-567.
- [Google Scholar]
- Substance abuse among adolescents in urban slums of Sambalpur. Indian J Community Med. 2008;33(4):265-267.
- [CrossRef] [Google Scholar]
- Tobacco smoking and its association with illicit drug use among young men aged 15-24 years living in urban slums of Bangladesh. PLoS One. 2013;8(7):e68728.
- [CrossRef] [Google Scholar]
- Prevalence and causes of substance abuse among undergraduate medical college students. Ind Med Gaz. 2014;148(8):276-82.
- [Google Scholar]



