

Translate this page into:
Disparities in Urban and Rural Dwelling Adolescents' Educational Needs for Obesity Prevention in Nigeria
✉Corresponding author email: soupriyezibima@gmail.com
Abstract
Background and Objectives:
Obesity has increased in recent times and has attained an epidemic status worldwide, incuding in Nigeria. Prevalence of obesity rises during adolescence and prevention is advantageous. However, it is unknown whether rural and urban dwelling adolescents in Bayelsa State in the Niger Delta region of Nigeria have the requisite knowledge needed to prevent obesity. The objective of this study was to determine the educational needs of urban and rural dwelling adolescents for obesity prevention.
Methods:
The study was a school-based cross-sectional survey, and employed multistage sampling technique to select six secondary schools across the three senatorial districts of the state. An adapted and validated sub-scaled obesity knowledge questionnaire was used to obtain data from 2,304 secondary school students. Statistical Package for Social Sciences (SPSS) version 23.0 was used for data analysis.
Results:
The total number of urban male students and rural male students was 576 (25.00%). The total number of urban female students and rural female students was also 576 (25.00%). The sample mean age of participants was 16.77 (SD±79), and those aged 16 years 1,043 (45.27%) were the largest portion of the sample. Generally, 756 (32.81%) of the participants had good knowledge of obesity. Specifically, subscale analysis showed that 622 (27.00%) participants had good knowledge of risk factors for obesity; 519 (22.53%) had good knowledge of complications of obesity; 659 (28.60%) had good knowledge of prevention for obesity; and 653 (28.34%) had good knowledge of meaning/assessment of obesity. Difference in mean score between urban (M= 3.80, SD = 0.44) and rural residents (M = 3.72, SD = 0.43; t = 4.63, p = 0.00, 2-tailed) was significant.
Conclusion and Implications for Translation:
Adolescents' knowledge regarding obesity is generally inadequate, especially in rural areas. Adolescents need education to acquire fundamental knowledge of the meaning/assessment, risk factors, prevention, and complications of obesity for prevention.
Keywords
Adolescent
Obesity Prevention
Bayelsa State
Niger Delta
Nigeria

Introduction
Obesity remains a serious public health problem worldwide.1 It is a chief contributor to many avoidable deaths in the world, and it is recognized as a powerful risk factor for common chronic diseases, such as hypertension, type 2 diabetes mellitus, gallbladder disease, cardiovascular diseases, renal diseases, sleep apnea, orthopedic complications, hyperlipidemia, and psychosocial disorders.2,3
In recent times, obesity has increased and attained an epidemic status.2,4 Between 1975 and 2016, the number of obese adults in the world has grown approximately three times higher to over 650 million.5 The number of obese adolescents and school-age children has also increased by three-fold compared to figures in 1980; while the number of overweight or obese children younger than 5 years increased to an estimated 41 million in 2016. 2,5
Obesity is also on the rise in Nigeria. According to the World Health Organisation (WHO), the prevalence of obesity in Nigeria has increased by 47% in men and 39% in women between 2002 and 2010.6 Other investigators have also reported high prevalence rates in different parts of Nigeria. In 2014, a study in Abuja, the nation's capital, reported a prevalence rate of overweight or obesity 64% (30% of women and 34% of men with a mean age of 42±9.3SD), while in 2018, another study in the Niger Delta Region, reported a prevalence rate of overweight or obesity 35.9% (6.1% of women and 29.8% of men with a mean age of 48±14.8SD).4,7 These reported prevalence rates tend to suggest that Nigeria shares significantly in the obesity pandemic, especially being the most populated country in Africa and the largest black nation in the world.
Obesity needs to be reduced urgently considering the marked increase in prevalent rates as well as its impact on health and economic development. Whereas obesity can be reduced through prevention and treatment, reduction strategies which are focused on prevention rather than treatment seem to be more advantageous in terms of cost of resources and sequel associated with treatment. Also, in view of obesity as a condition of energy imbalance, less behaviour change is needed to prevent weight gain, than to reverse obesity in those who are already obese.2
One of the strategies frequently recommended to prevent obesity is education of the populace. 4,7,8,9 Nevertheless, the scope of education that is relevant to specific populations or groups, needs to be known. This requires assessment of knowledge about obesity among such populations or groups as implementation of arbitrarily formulated preventive educational programs may not produce desired significant results. Such assessment is particularly necessary for an adolescent population as evidence suggests that the prevalence of obesity rises from age 20, and 80% of obese adolescents grow to become obese adults.10,11
In Nigeria and particularly Bayelsa State of the Niger Delta region, not much is known about obesity among urban and rural dwelling adolescents due to paucity of information. Therefore, gaining insight into educational needs that are specific to adolescents would assist in development of appropriate educational programs and formulation of preventive public policies that would facilitate behavior change, encourage healthy food choices, and enhance easy access to physical activity.
The objective of the study was to determine the educational needs for the prevention of obesity among adolescents dwelling in urban and rural areas of Bayelsa State, Nigeria. Our hypothesis was that there would be no significant difference in the knowledge of obesity between urban and rural dwelling adolescents.
Methods
Research Design
A school based cross sectional survey was done to assess what adolescents know about obesity. The multistage sampling technique was used for the study. At stage 1, the three senatorial districts in Bayelsa State were taken as clusters, making a total of three clusters. At stage 2, simple random sampling technique was employed by way of balloting to select one Local Government Area (LGA) in each of the clusters, making a total of three LGAs. At stage 3, the largest secondary school with both genders in the rural and urban part of each of the three LGAs was purposively selected, making a total of six secondary schools. The selected schools were then numbered 1 to 6 and students were reached at convenience. To determine the size of the sample, a confidence level of 95%, a ratio of 50% and an estimation error of 3.5% were considered, bringing the number of eligible students for the study to a total of 2,304 (384 from each school). Only students aged 16 and above were eligible.
Data Collection
Data were obtained with a 22-item obesity knowledge questionnaire adapted from the developers of Questionnaire for Assessment of Knowledge, Attitude and Practice of Obese Individuals about Obesity.12 The adapted questionnaire had two sections. Section One was comprised of three questions which were designated to obtain demographic data. Section Two consisted of nineteen questions based on a 5-point response scale of “Strongly Agree (SA), Agree (A), Disagree (D), Strongly Disagree (SD) and I do not know,” which assessed respondents' general knowledge of obesity. The nineteen 5-point response scale questions were further divided into four subscales. Items 1, 2, 3 and 4 of Section Two constitute the first subscale which assessed respondents' knowledge on meaning/ assessment of obesity; items 5, 6, 7, 8, 9, 10 and 11 constitute the second subscale which assessed knowledge of risk factors of obesity; items 12, 13, 14 and 15 constitute the third subscale which assessed knowledge of complications of obesity, and items 16, 17, 18, and 19 constitute the fourth subscale which assessed knowledge of prevention of obesity. The responses were weighted 5, 4, 3, 2 and 1 for SA, A, D, SD and I do not know, respectively. The lowest and highest obtainable scale score for general knowledge of obesity is 1 and 95 respectively. Similarly, the lowest obtainable score for subscales is 1 while the highest obtainable score depended on the number of items that make up the subscale.
The adapted instrument was tested for reliability and validity through test retest method and subject expert analysis respectively. The computed Pearson Product Moment Correlation Coefficient (r) was 0.89 while the Scale Content Validity Index (S-CVI) of the expert analysis was 0.9. Fifteen (15) minutes only of respondents' break period was used each day for questionnaire administration to avoid disruption of learning activities.
Statistical Analysis
Descriptive statistics was done with the Statistical Package for Social Sciences (SPSS) version 23.013 to generate frequencies, percentages, means and standard deviations of data collected. Means of total knowledge scores and scores on the four (4) knowledge subscales were computed and classified as poor, fair and good knowledge depending on the cut off points. Independent samples t-test at 95% confidence interval (CI) and p-value ≤ 0.05, was conducted to compare difference in the mean scores of general knowledge of obesity, between urban and rural dwelling adolescents. Eta square was further computed to determine the effect size of existing difference. Ethical approval and administrative permits were obtained from the Bayelsa State Ministry of Education and the schools' Headmasters respectively. Adolescents who had attained 18 years gave verbal consent while, the class teachers who also assume parental role during school periods when the students are in their custody, gave verbal consent for adolescents below 18 years.
Results
Sociodemographic Characteristics of the Study Participants
A total of 2,304 adolescents in secondary schools participated in the study. The sample mean age of respondents was 16.77(SD±79). Those aged 16(1,043/45.27%) were more than those aged 17 (752/32.64%) and 18 (509/22.09%). Equal proportion of males (1,152/50.00%) and females (1,152/50.00%) in both rural (1,152/50.00%) and urban (1,152/50.00%) locations were sampled (Table 1).
| (N = 2,304) | Frequency (n) | Percentage (%) |
|---|---|---|
| Age | ||
| 16 years | 1,043 | 45.26 |
| 17 years | 752 | 32.64 |
| 18 years | 509 | 22.09 |
| Mean Age | 16.77 (SD±79) | |
| Gender | ||
| Male | 1,152 | 50.00 |
| Female | 1,152 | 50.00 |
| Residential location | ||
| Rural | 1,152 | 50.00 |
| Urban | 1,152 | 50.00 |
Knowledge of Obesity
Scores on general knowledge of obesity showed that 790 (34.28%), 758 (32.89%) and 756 (32.81%) had poor, fair and good knowledge, respectively (Figure 1). Also, measures on knowledge subscales showed that less than one-third of the respondents had good knowledge in all the four areas assessed. Specifically, only 653 (28.34%) had good knowledge of meaning/assessment of obesity; 622 (27.00%) had good knowledge of risk factors of obesity; 519 (22.53%) had good knowledge of complications of obesity and 659 (28.60%) had good knowledge on the prevention of obesity (Table 2).
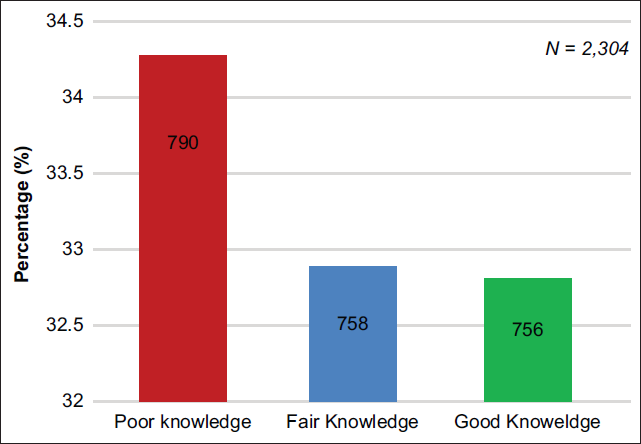
- Level of General Knowledge of Obesity among Adolescents. Scores on Knowledge Scale ranging from 1 -68 = Poor Knowledge; 69 – 74 = Fair Knowledge and 75 - 95 = Good knowledge
| Levels of knowledge | Knowledge of meaning/ assessment of obesity Total scale score=20 (N/%) | Knowledge of risk factors of obesity Total scale score =35 (N/%) | Knowledge of complications of obesity Total scale score=20 (N/%) | Knowledge of prevention of obesity Total scale score=20 (N/%) |
|---|---|---|---|---|
| Poor | 946 (41.06%) | 831 (36.06%) | 893 (38.75%) | 778 (33.77%) |
| Fair | 705 (30.60%) | 851 (36.94%) | 892 (38.72%) | 867 (37.63%) |
| Good | 653 (28.34%) | 622 (27.00%) | 519 (22.53%) | 659 (28.60%) |
Scores on Knowledge of Meaning/Assessment of Obesity Subscale range from 1 -15 = Poor Knowledge; 16 – 17 = Fair Knowledge; and 18 -20 = Good knowledge
Scores on Knowledge of Risk Factors of Obesity Subscale range from 1 – 25 = Poor Knowledge; 26 – 29 = Fair Knowledge and 30 -35 = Good knowledge
Scores on Knowledge of Complications of Obesity Subscale range from 1-14 = Poor Knowledge; 15 – 16 = Fair Knowledge and 17 -20 = Good knowledge
Scores on Knowledge of Prevention of Obesity Scale range from 1 -13 = Poor Knowledge; 14 – 15 = Fair Knowledge and 16 -20 = Good knowledge
Knowledge Difference between Rural and Urban Dwelling Adolescents
An independent samples t-test computed to compare scores on knowledge of obesity between urban and rural dwelling adolescents, indicated that, significant difference exists between urban (M= 3.80, SD = 0.44) and rural residents (M = 3.72, SD = 0.43; t (2,304) = 4.63, p = 0.00, 2-tailed). However, effect size which was determined through eta square showed that the magnitude of difference was small (0.01) (Table 3).
| Residential location | N | Mean (m) | Standard deviation (sd) | T | Df | Sig. (2-Tailled) | 95% CI | Eta squared |
|---|---|---|---|---|---|---|---|---|
| Urban | 1,152 | 3.80 | 0.44 | 4.63 | 2302 | < 0.05 | 0.05 – 0.12 | 0.01 |
| Rural | 1,152 | 3.72 | 0.43 | |||||
Discussion
Knowledge of obesity has been assessed in previous studies among adolescents of different ages; usually between 14 and 20 years.1,14,15 In this study, only adolescents aged 16 and above were considered and results showed that most (45.27%) of the adolescents were at age 16 and none was up to 20 years. The choice of age 16 and above was made because we premised that most adolescents within this age range are considerably older to already be in senior secondary school classes and therefore, may comparatively have better comprehension of the assessment test.16 More so, age 16 and above fall within the population age in which obesity is reportedly rising astronomically.10,11
In terms of knowledge on obesity, findings showed that respondents were not ignorant of obesity and its prevention even though the knowledge content was variable among them. Most of the adolescents generally had fair and good knowledge (758/2,304 and 756/2,304 respectively), findings which are similar to reports that adolescent students generally have different levels of knowledge about obesity.14-15,17,18 However, a substantial proportion of the respondents demonstrated poor knowledge when separately assessed on different aspects of obesity, such as the meaning/assessment of obesity (0.41), risk factors of obesity (0.36), complications of obesity (0.39) and prevention of obesity (0.34). These findings agree with the report that knowledge of many adolescents regarding obesity is below average.15,17,18 It also shows that there is lack of adequate knowledge of obesity and its prevention among adolescents as is similarly reported in literature.15 The implication is that, adolescents are at risk of developing obesity and its attendant complications as they may not take necessary steps to prevent it. There is, therefore, need for proper adolescent education on the meaning/assessment of obesity, risk factors of obesity and the complications and prevention of obesity.
Gender-based reports regarding superiority of knowledge of obesity among adolescent students also exist, 1,18 but this study did not elicit any discrepancy of such. However, urban dwelling adolescent students were found to have more knowledge of obesity and its prevention than those in rural areas. This finding is congruent with available literature1 and the reason may not be unconnected with availability of modern facilities, technologies and mass media that the students may be exposed to. Through such media, they may have heard electronic teachings and adverts that increased their knowledge above their rural counterparts who may not have electricity and other electronic facilities that would enhance their learning and experience.
Although, the non-inclusion of adolescents in private secondary schools tend to limit this study, its strength, however, lies in the fact that public secondary schools which accommodate the majority of adolescents in the three senatorial districts of the state were included. Thus, findings could validly be generalized within the study milieu and by extension to similar populations elsewhere. Future research should, however, expand samples to include adolescents in private secondary schools.
Conclusion and Implications for Translation
Based on the foregoing, it can be concluded in this study that knowledge about obesity among adolescents is generally inadequate, especially those in rural areas. Adolescents need education to acquire fundamental knowledge on the meaning/assessment of obesity, risk factors of obesity, prevention of obesity and the complications of obesity in order to be able to prevent it. We, therefore, suggest that the findings of this study and similar ones be disseminated to teachers and heads of schools where adolescents are found in order to stimulate them to incorporate lessons on obesity in their teachings. Government, through the Ministry of Education, should include obesity as a topic in the curriculum so that widespread teaching of it can be encouraged. Public sensitization campaigns on adolescent obesity and its prevention are also necessary to improve their knowledge.
Compliance with Ethical Standards
Conflicts of Interest:
The authors declare that they have no conflict of interest.
Financial Disclosure:
None.
Ethics Approval:
Prior to the study, ethical approval and administrative permit were obtained from the Bayelsa State Ministry of Education and the Headmasters of the selected secondary schools to participate in the study and the data obtained were confidentially handled.
Disclaimer:
None.
Acknowledgments:
The teachers and students of the secondary schools where the study was done are sincerely acknowledged for their support and cooperation.
Funding/Support:
There was no funding for this study.
References
- Knowledge and attitude regarding obesity among adolescents of Sikar, Rajasthan. IOSRJ Nurs Health Sci. 2014;3(2):44-48.
- [CrossRef] [Google Scholar]
- Modern Nutrition in Health and Disease (11th). Wolters Kluwer Health; 2014.
- Complications of obesity in adults: A short review of the literature. Malawi Medical Journal. 2014;26(1):20-24.
- [Google Scholar]
- Obesity epidemic has emerged among Nigerians. BMC Public Health. 2014;14:455.
- [CrossRef] [PubMed] [Google Scholar]
- 2018. Fact Sheet on Overweight and Obesity. (accessed )
- 2012. WHO global comparable estimates: Global infobase data for saving lives 2005. (accessed )
- Screening for obesity during the World Health Day in Ogboloma, a small rural settlement in the Niger Delta region of Nigeria. J Adv Med Med Res. 2018;26(6):1-8.
- [CrossRef] [Google Scholar]
- Assessment of the prevalence of obesity in Idema Community, Ogbia Local Government Area of Bayelsa State. Asian Pacific J Health Sci. 2015;2(2):20-24.
- [CrossRef] [Google Scholar]
- Prevalence of overweight and obesity among adolescents in secondary schools in Abia State, Nigeria. Annu Res Rev Biol. 2015;5(5):433-438.
- [CrossRef] [Google Scholar]
- Obesity in North America. An overview. Med Clin North Am. 2000;84(2):305-332.
- [CrossRef] [PubMed] [Google Scholar]
- Body mass index during childhood, adolescence and young adulthood in relation to adult overweight and adiposity: the Fels Longitudinal Study. Int J Obes Relat Metab Disord. 2000;24(12):1628-1635.
- [CrossRef] [PubMed] [Google Scholar]
- Development and validation of a questionnaire assessing knowledge, attitude, and practices about obesity among obese individuals. Indian J Endocrinol Metab. 2019;23(1):102-110.
- [CrossRef] [PubMed] [Google Scholar]
- IBM Corp released 2015. IBM SPSS Statistics for Windows, Version 23.0. Armonk NY: IBM Corp;
- [Google Scholar]
- Assessment of knowledge about obesity among students in a medical college in Kancheepuram district, Tamil Nadu. Prog Health Sci. 2013;3(1):54-60.
- [Google Scholar]
- A study to assess the knowledge and attitude of adolescents on obesity at selected senior secondary schools in Amristar in a view to develop and distribute information booklet. Int J Educ Appi Res. 2014;4(1):35-39.
- [Google Scholar]
- Effect of age and gender on children's reading performance: the possible neural underpinnings. Cogent Psych. 2015;2(1)
- [CrossRef] [Google Scholar]
- A descriptive study to assess the knowledge regarding obesity and its ill- effect on health among adolescent girls, in selected college of Indore, M.P. Int J Adv Res Ideas Innovations Technol. 2018;4:979-983.
- [Google Scholar]
- A study to assess the knowledge and proportion of obesity among High school children in selected schools of Hyderabad, Telangana. Int J Adv Res Med Pharm Sci. 2017;2(11):1-6.
- [Google Scholar]



