

Translate this page into:
Ocular Health Complications Among People Living with HIV/AIDS in Nigeria: Leveraging Doppler Ultrasonography to Identify and Manage Risk Factors
 MBBS, MSc, Mohammed Kabir Saleh2MBBS, MSc, Yahuza Mansur Adamu2MBBS, Sadiq Hassan3MBBS, Muktar Hassan Aliyu4MD, MPH, DrPH, Anas Ismail2MBBS, MD
MBBS, MSc, Mohammed Kabir Saleh2MBBS, MSc, Yahuza Mansur Adamu2MBBS, Sadiq Hassan3MBBS, Muktar Hassan Aliyu4MD, MPH, DrPH, Anas Ismail2MBBS, MD

*Corresponding author: Ahmad Bashir Umar, Department of Radiology, Aminu Kano Teaching Hospital, PMB 3452, Zaria Road, 700233, Kano State, Nigeria, abashir4@hotmail.com
-
Received: ,
Accepted: ,
How to cite this article: Umar AB, Saleh MK, Adamu YM, Hassan S, Aliyu MH, Ismail A, et al. Ocular health complications among people living with HIV/AIDS in Nigeria: Leveraging Doppler ultrasonography to identify and manage risk factors. Int J Transl Med Res Public Health. 2025;9:e002. doi: 10.25259/IJTMRPH_69_2024
Abstract
Background and Objective
HIV-associated retinopathy and other ocular complications remain conditions of concern despite the introduction of combination antiretroviral therapy (ART). Evaluating people living with HIV (PLWH) for early hemodynamic changes in their ophthalmic arteries using Doppler ultrasonography is crucial to modifying care and preventing potential retinal damage.
Methods
This case-control study included 150 eligible adults on ART and an equal number of age- and sex-matched apparently healthy HIV-negative controls. We performed a comprehensive ocular examination and determined Doppler velocimetric indices (resistive and pulsatility index) in both ophthalmic arteries using a 7.5 MHz transducer.
Results
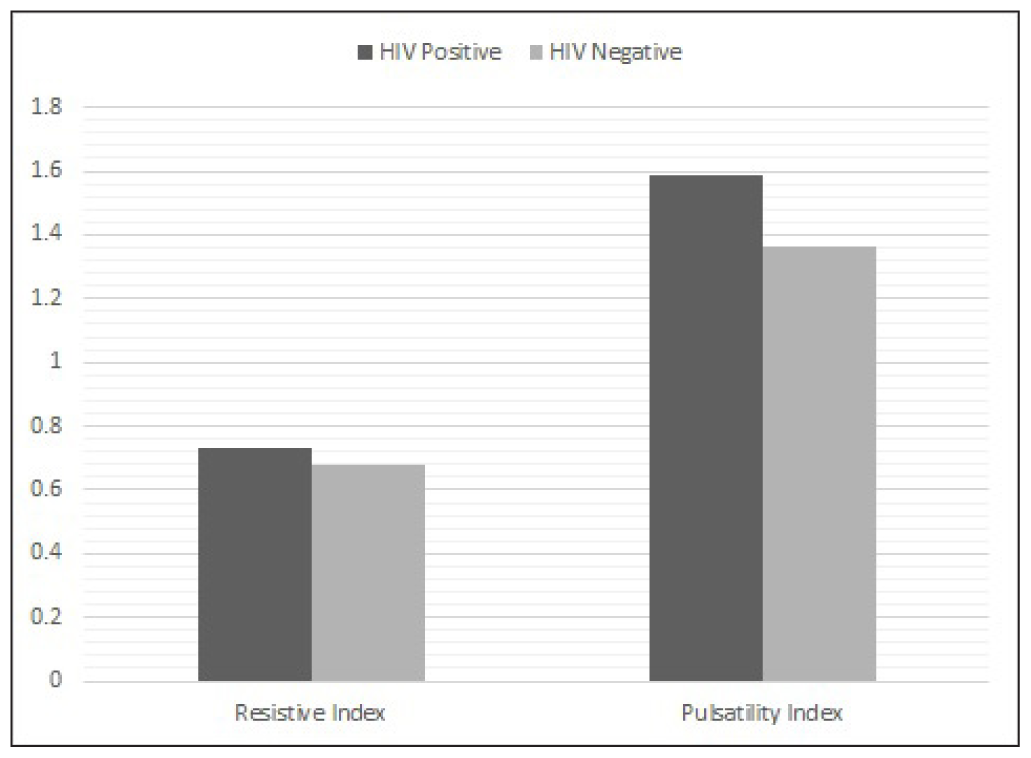
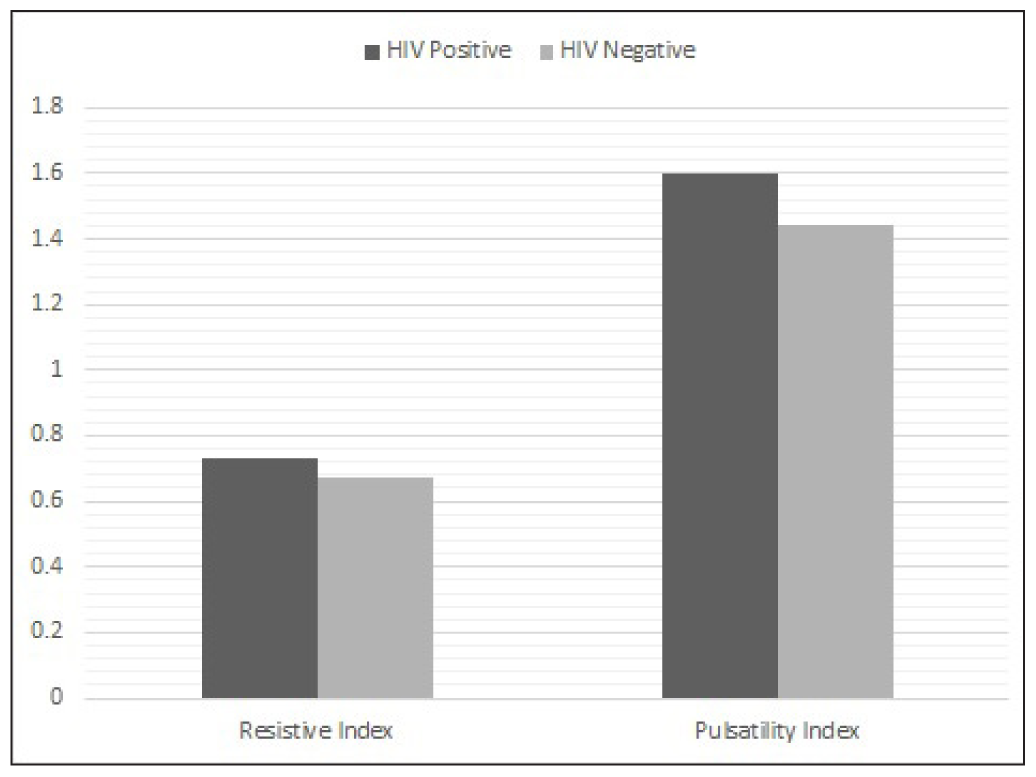
A total of 300 participants were included, of which 48% were males and 52% were females. The overall mean age (±standard deviation, SD) of participants was 41 ± 10 years. The prevalence of ocular abnormalities via fundoscopy was 13% among PLWH and 2% in the control group. The mean ophthalmic artery resistive indices (±SD) for HIV-positive participants were 0.73 (±0.05) in the right eye and 0.73 (±0.04) in the left eye, both higher than that of the apparently healthy controls at 0.68 (±0.05) and 0.67 (±0.05) in the right and left eyes, respectively. Similarly, the mean right and left ophthalmic artery pulsatility indices were higher among PLWH than controls (1.59 ± 0.35 and 1.60 ± 0.33 compared to 1.36 ± 0.33 and 1.44 ± 0.98, respectively).
Conclusion and Implications for Translation
Ocular abnormalities are common among PLWH. Ophthalmic artery Doppler indices were significantly higher among PLWH than age- and sex-matched healthy controls, indicating some form of ocular vascular resistance. We recommend regular ocular examinations for PLWH in similar settings.
Keywords
Antiretroviral Therapy
Doppler Ultrasonography
Hemodynamics
HIV
Ophthalmic Artery
Vascular Resistance

INTRODUCTION
Inflammatory intraocular conditions are common in people living with HIV and are often due to opportunistic infections like cytomegalovirus (CMV) retinitis, ocular syphilis or tubercular uveitis, and neoplasms, such as intraocular lymphoma, and immune recovery uveitis.[1] The introduction of CMV-specific anti-viral medications and combination antiretroviral therapy (ART) significantly decreased the incidence of CMV-related vision loss, but new conditions, such as immune reconstitution inflammatory syndrome (IRIS), emerged.[2] Retinal toxicity has also been associated with the use of antiretroviral drugs, such as efavirenz.[3] Noninfectious co-morbidities such as coronary artery disease, osteoporosis, chronic kidney disease, hyperlipidemia, liver disease, and non-AIDS-defining malignancies have also become more common since the introduction of ART, and some of them contribute to vision loss.[2] As a result, especially in the aging population, the emphasis on ocular care for HIV-infected patients has shifted from the management of acute disease to care for chronic conditions.
The advent of Doppler ultrasonography has added a dynamic dimension to ocular ultrasonography. In this technique, sonography is enhanced with Doppler measurements, which employ the Doppler effect in studying the kinetics of blood flow in intra-ocular, orbital, and carotid vessels.[4] The use of ART is implicated in the reduction of ocular blood flow.[5] Thus, the use of non-invasive and non-ionizing radiation-based imaging modalities like ultrasonography can play a role in evaluating PLWH on ART. Due to its relative availability over alternative imaging techniques, ocular ultrasonography is an ideal imaging tool in the resource-limited settings of low- and medium-income countries.[6]
Early evaluation of PLWH for ocular hemodynamic changes is important for preventing irreversible retinal damage and maintaining their quality of life. Doppler ultrasonography, which is both safe and sensitive, can be used to assess these changes. Measuring velocimetric indices such as peak systolic velocity (PSV), end-diastolic velocity (EDV), resistive index (RI), and pulsatility index (PI) in the ophthalmic arteries of PLWH and comparing these measurements with those of seronegative healthy controls will help us to better understand how to modify care and reduce the risk of retinal damage in PLWH.
METHODS
This hospital-based case-control study was conducted at the HIV treatment center of Aminu Kano Teaching Hospital in northern Nigeria over 6 months. One hundred and fifty adults with HIV on ART and equal number of age-and sex-matched healthy seronegative participants were recruited following a stratified sampling method. A sample size of 150 for each of the groups was obtained using the sample size formula for a two-sample t-test,[7] with an alpha level of 0.05 and standard normal deviation corresponding to a power of 80%. The mean and standard deviations of resistive indices in the ophthalmic arteries from previous studies[8, 9] of HIV-positive subjects and healthy controls were substituted into the formula to arrive at this sample size.
Participants
The inclusion criteria for the study group include age >18 years, proven HIV infection (positive ELISA test), and being on ART. For the control group, persons older than 18 years of age and proven to be seronegative for HIV infection on an enzyme-linked immunosorbent assay (ELISA) test were enrolled. We excluded those diagnosed with hypertension or diabetes mellitus, a history of any eye disease that may affect blood flow, such as ocular inflammation, glaucoma, or uveitis, and history of trauma to the orbits, active AIDS-defining illness, alcohol abuse, and cigarette smokers (smoking more than five cigarettes in a day in the preceding year), as well as those who did not give consent. The age, sex, body mass index (BMI), and blood pressure for both the cases and control participants were determined and documented. The CD4+ counts and HIV RNA viral load baseline were also obtained accordingly. The viral load was categorized into undetectable = <50 copies/ml, low = 50 – 1000 copies/ml, and high = >1000 copies/ml. The CD4 count as a reflection of immune deficiency was classified into “Severe” = <200 cells/mm3, “Advanced” = 200 –3 49 cells/mm3, “Mild” = 350 – 499 cells/mm3, and “Not significant” = >500 cells/mm3.
Study Procedure
The participants underwent a comprehensive ocular examination and Doppler ultrasonography to evaluate the ophthalmic arteries. A Nortek Digital Ultrasound Imaging System (Model CS-50, Nortek Healthcare Electronics, Shenzen, China) equipped with a 7.5 MHz linear transducer was used for the ocular Doppler sonography. A trained consultant radiologist with more than 5 years of experience in vascular imaging obtained the Doppler velocimetric indices. To evaluate intraobserver reliability, measurements were repeated three times, and the average was recorded by a single observer. To assess measurement consistency, we computed the intra-class correlation coefficient (ICC) for 20 randomly selected subjects, with measurements taken by a single observer 2 weeks apart. The resulting ICC was >0.7, indicating good reliability.
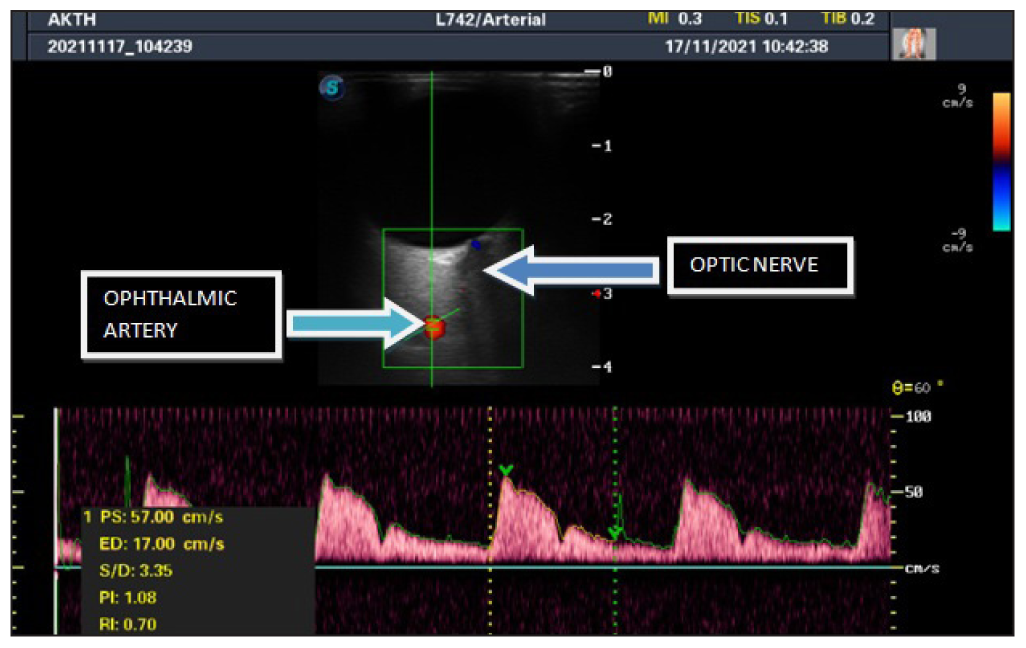
The participants were placed in a supine position and their heads tilted at an angle of about 30° with the eyes closed.[10] An acoustic coupling gel was then applied to the transducer, which was then placed directly and gently on the closed eyelid with the gaze directed at the ceiling.[11] The examiner’s hand was rested on the orbital margin to minimize the applied pressure to the eye globe and the orbit.[10] The angle of the transducer was set at 30° to 60° during the course of the examination. Real-time grayscale and color Doppler scanning were then performed in the longitudinal and transverse planes of both globes. The hypoechoic stripe of the optic nerve was then identified with the ophthalmic artery just lateral to it.[12] Color Doppler imaging was performed with the gain adjusted to avoid artifactual color noise, thus allowing detection of low velocities.[10] The blood flow velocity of the ophthalmic artery was measured nasally directly after crossing the optic nerve approximately 2–3 cm behind the globe, and based on the vessel course, an angle correction was applied between the transducer and the vessel. The Doppler sample gate (≤2 mm) was placed at the center of the detected vessel to image the spectral pattern.[13] The spectral waveform as well as the velocimetric indices which include Peak systolic velocity (PSV), End diastolic velocity (EDV), Resistive index (RI), Pulsatility Index (PI), and S/D ratio were obtained and recorded [Figure 1].
Before the commencement of the fundoscopic examination, visual acuity with a Snellen chart (alphabetical) as well as an examination of the anterior segment with a Haag-Streit slit lamp was conducted by a consultant ophthalmologist. Intra-ocular pressure was measured with an applanation Tonometer (Haag-Streit international AT-900). A single experienced ophthalmologist conducted the fundoscopic examination throughout the study to prevent inter-observer variability. The participant was made as comfortable as possible during the examination. The light of the room was dimmed, and a mydiatric agent (Tropicamide 1%) was applied and allowed for at least 15–20 minutes for adequate pupillary dilation.[14] The participant was then instructed to look at a distant target. The ophthalmologist stood at the side of the participant, using the left eye and hand to examine the participant’s left eye and vice versa with the free hand on the subject’s forehead and using the thumb to hold the upper eyelid open if necessary. The field of view of the fundus was adjusted based on the distance to the participant’s eye. Following the red reflex exam, the optic disc was evaluated by moving the field of view along the apex of a branching blood vessel. Thereafter, the retinal blood vessels, macula, and peripheral fundus were examined using a non-contact Volk condensing lens (+90D) and the slit lamp.[14] The presence or absence of the following was evaluated: microaneurysms, cotton wool spots, optic disc edema, and intraretinal hemorrhages.
Statistical Analysis
The data were analyzed using SPSS version 22.0 (IBM Corp., Armonk, NY, 2013). Continuous variables were reported as the mean ± standard deviation (SD), and categorical factors were reported as percentages. The Chi-square test was used to assess associations between fundoscopic findings and viral load or CD4 count. We used Pearson correlation analysis to examine the relationship between Doppler velocimetric indices and duration of ART and viral load. We employed a one-way ANOVA to compare the means of Doppler velocimetric indices across different ART drug combination regimens. Logistic regression was used to evaluate the correlation between the Doppler velocimetric indices and fundoscopic examination findings. A p-value of equal to or less than 0.05 was considered statistically significant.
RESULTS
Three hundred participants were included in the study, comprising 150 HIV-infected adults on ART and an equal number of HIV-negative age- and sex-matched controls. Seventy-two participants (48%) were males and seventy-eight (52%) were females in each of the groups. The age range of the HIV-positive participants was 18–70 years with a mean age of 41.2 ± 10.3 years, while that of the HIV-negative control participants was 18–69 years with a mean of 41.2 ± 10.2 years (p = 0.215), as shown in Table 1. The majority (78.7%) of HIV-positive participants had undetectable viral load ≤50 copies/ml and normal CD4 counts ≥500 cells/mm3. There was a statistically significant relationship between fundoscopic findings and viral load/CD4 count among the HIV-positive participants in the study [Table 2].
| Variables | HIV positive on ART n = 150 (%) | HIV negative Control n = 150 (%) |
|---|---|---|
| Age (years) | ||
| 18–27 | 14 (9.3) | 14 (9.3) |
| 28–37 | 40 (26.7) | 40 (26.7) |
| 38–47 | 55 (36.7) | 56 (37.3) |
| 48–57 | 31 (20.7) | 31 (20.7) |
| >57 | 10 (6.7) | 9 (6.0) |
| Mean ± SD | 41.2 ± 10.3 | 41.2 ± 10.2 |
| Gender | ||
| Male | 72 (48.0) | 71 (47.3) |
| Female | 78 (52.0) | 79 (52.7) |
| Duration of ART (years) | ||
| <5 | 19 (12.7) | - |
| 5–10 | 60 (40.0) | - |
| 11–15 | 55 (36.7) | - |
| 16–20 | 13 (8.7) | - |
| >20 | 3 (2.0) | - |
| Viral load (copies/ml) | ||
| Undetectable | 118 (78.7) | - |
| Low | 28 (18.7) | - |
| High | 4 (2.7) | - |
ART: Antiretroviral therapy, SD: Standard deviation,
| Fundoscopic findings | |||
|---|---|---|---|
| Normal | Abnormal | Total (%) | |
| Viral load | |||
| Undetectable | 109 (72.7) | 9 (6.0) | 118 (78.7) |
| Low | 20 (13.3) | 8 (5.3) | 28 (18.7) |
| High | 1(0.7) | 3 (2.0) | 4 (2.7) |
| p-value <0.001* | |||
| CD4+ count | |||
| Not significant | 113 (75.3) | 11 (7.3) | 124 (82.7) |
| Mild | 11 (7.3) | 6 (4.0) | 17 (11.3) |
| Advanced | 5 (3.3) | 1 (0.7) | 6 (4.0) |
| Severe | 1 (0.7) | 2 (1.3) | 3 (2.0) |
| p-value <0.001* | |||
*Significant at p ≤ 0.05.
Among the 150 HIV-positive participants, the most common antiretroviral regimen (71.3%) was Dolutegravir/Lamivudine/Tenofovir, followed by Tenofovir/Lamivudine/Atazanavir at 12.7% [Table 3]. The majority (87%) of the HIV-positive participants on ART had normal fundoscopic examination findings. The most common abnormal ocular findings were cotton wool spots and optic disc changes suspicious for glaucoma, at 3.3% each. Retinal hemorrhage and microaneurysms were seen in 1.3% of HIV-positive participants [Table 3]. Among the HIV-negative participants, the majority (98%) had normal fundoscopic findings, while 2% had a suspicion of glaucoma.
The ophthalmic artery PSV, EDV, RI, and PI values for both the case and control groups are shown in Table 4. The differences in Doppler indices between the HIV-positive and HIV-negative subjects were statistically significant [Table 4]. The mean RI and PI values among the HIV-positive subjects were higher than those of the HIV-negative control group for both the right and left eyes, as shown in Figures 2 and 3, and this difference was also statistically significant (p < 0.001).
Participants on the ABC/3TC/DTG (Abacavir/Lamivudine/Dolutegravir) regimen had the highest mean resistance index (RI) of 0.75 ± 0.04 in both eyes. In contrast, those on AZT/3TC/LPV/r (Zidovudine/Lamivudine/Lopinavir) had the lowest mean RI, with values of 0.72 ± 0.04 for the right eye and 0.072 ± 0.03 for the left eye. However, there was no statistically significant difference between the mean RI and PI of participants on the different ART drug regimens [Table 5]. Logistic regression analysis revealed no statistically significant association between the resistive index (RI) and pulsatility index (PI) of the ophthalmic arteries among the HIV-positive participants on ART.
| Variable | n = 150 | (100.0%) |
|---|---|---|
| ART regimen | ||
| DTG/3TC/TDF (Dolutegravir/Lamivudine/Tenofovir) | 107 | 71.3 |
| AZT/3TC/ATV/r (Zidovudine/Lamivudine/Atazanavir) | 11 | 7.3 |
| AZT/3TC/LPV/r (Zidovudine/Lamivudine/Lopinavir) | 7 | 4.7 |
| AZT/3TC/NVP (Zidovudine/Lamuvidine/Nevirapine) | 1 | 0.7 |
| TDF/3TC/ATV/r (Tenofovir/Lamivudine/Atazanavir) | 19 | 12.7 |
| ABC/3TC/DTG (Abacavir/Lamivudine/Dolutegravir) | 5 | 3.3 |
| Fundoscopic findings | ||
| Suspected CMV retinitis | 1 | 0.7 |
| Cotton wool spots | 5 | 3.3 |
| Optic disc changes suspicious for glaucoma | 5 | 3.3 |
| Macular edema | 1 | 0.7 |
| Normal | 130 | 86.7 |
| Papilloedema | 1 | 0.7 |
| Retinal hemorrhage | 2 | 1.3 |
| Retinal microaneurysm | 2 | 1.3 |
| Uveitis | 3 | 2.0 |
ART: Antiretroviral therapy, CMV: Cytomegalovirus.
| Variables | HIV-positive on ART | HIV-negative controls | p-value | ||
|---|---|---|---|---|---|
| Right eye | Left eye | Right eye | Left eye | ||
| PSV (cm/s) | 14.3 – 95.63 | 14.21 – 100.72 | 14.09 – 90.72 | 14.21 – 88.98 | |
| EDV (cm/s) | 4.10 – 32.39 | 4.81 – 31.55 | 4.44 – 31.55 | 4.81 – 32.61 | |
| RI | 0.60 – 0.91 | 0.61 – 0.82 | 0.54 – 0.81 | 0.50 – 0.79 | |
| Mean ± SD | 0.73 ± 0.05 | 0.73 ± 0.04 | 0.68 ± 0.05 | 0.67 ± 0.05 | *<0.001 |
| PI | 0.91 – 3.33 | 0.90 – 3.31 | 0.68 – 2.24 | 0.61 – 2.27 | |
| Mean ± SD | 1.59 ± 0.35 | 1.60 ± 0.33 | 1.36 ± 0.33 | 1.44 ± 0.98 | *<0.001 |
*Significant at p ≤ 0.05; PSV: Peak systolic velocity; EDV: End diastolic velocity; RI: Resistive index; PI: Pulsatility index, ART: Antiretroviral therapy. SD: Standard deviation.
| ART drug regimen | RT_ RI | LT_RI | RT_PI | LT_PI |
|---|---|---|---|---|
| DTG/3TC/TDF | 0.73 ± 0.05 | 0.73 ± 0.05 | 1.59 ± 0.36 | 1.59 ± 0.34 |
| AZT/3TC/ATV/r | 0.74 ± 0.07 | 0.74 ± 0.06 | 1.60 ± 0.35 | 1.59 ± 0.31 |
| AZT/3TC/LPV/r) | 0.72 ± 0.04 | 0.72 ± 0.03 | 1.53 ± 0.31 | 1.52 ± 0.28 |
| AZT/3TC/NVP | 0.75 | 0.73 | 1.41 | 1.45 |
| TDF/3TC/ATV/r | 0.74 ± 0.05 | 0.74 ± 0.03 | 1.63 ± 0.42 | 1.72 ± 0.29 |
| ABC/3TC/DTG | 0.75 ± 0.04 | 0.75 ± 0.04 | 1.69 ± 0.25 | 1.74 ± 0.43 |
| p-value | 0.801 | 0.548 | 0.957 | 0.565 |
*Significant at p ≤ 0.05; RT: Right eye, LT: Left eye, RI: Resistive index, PI: Pulsatility index, ART: Antiretroviral therapy, ANOVA: Analysis of variance, DTG: Dolutegravir, 3TC: Lamivudine, TDF: Tenofovir, AZT: Zidovudine, ATV/r: Atazanavir, LPV/r: Lopinavir, NVP: Nevirapine, TDF: Tenofovir, ABC: Abacavir.
DISCUSSION
HIV infection is a multisystemic disease with worldwide distribution affecting various organs, including the human eye.[15] Ocular manifestations of HIV are often related to microvascular dysfunction and advanced stages of the disease. However, with the introduction of combination ART and increasing concerns about immune reconstitution inflammatory syndrome (IRIS), ocular hemodynamic changes can occur even in individuals with minimal or no symptoms, potentially leading to long-term complications, such as blindness.[16] Non-invasive imaging modalities, such as ocular Doppler ultrasonography, are valuable for detecting these hemodynamic changes at early stage. Studies have reported that resistive and pulsatility indices of the ophthalmic arteries are higher in HIV-positive patients on ART when compared to apparently healthy individuals, suggesting an increase in ocular vascular resistance.[5]
Several studies have found an inverse relationship between CD4+ count and vision-threatening ocular symptoms.[17–19] In this study, approximately 13% of HIV-positive participants exhibited ocular abnormalities on fundoscopy, with the majority (87%) having normal fundoscopic results. This could be attributed to the fact that ocular abnormalities are more common in advanced stages of HIV/AIDS, and most participants in this study were asymptomatic with high CD4+ counts and undetectable viral loads, explaining the high proportion of normal fundoscopic findings. In contrast, Martin-Odoom et al.[20] in Ghana reported a 48% prevalence of HIV-related ocular manifestations, likely because the majority of the participants in their study were symptomatic and in World Health Organization (WHO) stage III disease. Similarly, Arowolo et al.[21] in Port Harcourt, Nigeria, reported a 37% prevalence, possibly because they included participants not on ART in their study.
The mean ophthalmic artery resistive index (RI) among HIV-positive individuals on ART in this study was 0.73 in both eyes. This value was slightly higher than the 0.70 reported by Ajulo et al.[22] in Uyo, Akwa-Ibom, Southern Nigeria, where the participants were predominantly pediatric, with a mean age of 4.71 ± 0.59 years. Additionally, the mean RI in this study was slightly higher than the 0.70 recorded by Fabbiani et al.[5] in Rome and Grima et al.[8] in Galatina, Italy. The differences may be attributed to variations in ultrasound equipment and the inclusion of participants with co-morbidities such as dyslipidemia and a history of cigarette smoking in Italian studies. In contrast, Dejaco-Ruhswurm et al.[23] In Vienna, Austria, reported a higher mean RI of 0.79 among HIV-positive adults. This discrepancy could be due to their smaller sample size of 37 compared to the 150 participants in this study. There was no statistically significant relationship found between the mean RI and different ART drug regimens in this study, highlighting a gap in the literature that this study aimed to address.
Our study has strengths. To our knowledge, this is the first study from Nigeria to compare ophthalmic artery velocimetric indices between HIV-positive individuals on ART and healthy HIV-negative controls. We also used standardized approaches to measuring the velocimetric indices, improving the validity of our results. In addition, the relatively large sample size increases the generalizability of our findings. A limitation of the study is the fact that Doppler ultrasonography is user-dependent; as such, there may be variations in readings obtained depending on user skill and experience.
CONCLUSION AND IMPLICATIONS FOR TRANSLATION
We found that ocular vascular resistance, as determined by Doppler velocimetric indices, is significantly higher in HIV-positive adults on ART who had an average ophthalmic artery resistive index of 0.73 in both eyes compared to controls who had 0.67 and 0.68 on the right and left eye, suggesting a potential increased risk of retinal damage over time. In addition, consistent with other studies, we found that ocular abnormalities among HIV-positive adults on ART, as assessed by fundoscopy, were associated with viral load and CD4+ count. Our study highlights the elevated ocular vascular resistance in HIV-positive Nigerians on ART, suggesting a potential risk for retinal damage that warrants early detection and management. Our study contributes valuable regional data that emphasizes the need for regular eye examinations in people living with HIV and can be used to guide better clinical practice for monitoring HIV-related ocular complications.
Key Messages
1. Ocular Abnormalities in person living with HIV (PLWH): Increased prevalence of cotton wool spots and optic disc changes highlights the need for regular eye exams. 2. Elevated Doppler Indices: HIV-positive individuals on ART exhibit higher resistive and pulsatility indices, indicating greater ocular vascular resistance. 3. Immune and Viral Status Link: Ocular findings correlate with viral load and CD4+ count, stressing the role of immune status in eye health. 4. ART Regimens and Doppler Indices: No significant differences in Doppler indices across ART regimens suggest underlying HIV pathology as the main driver. 5. Early Detection Value: Doppler ultrasonography is a key non-invasive tool for identifying subclinical ocular changes and preventing retinal damage. 6. Regional Research Contribution: Provides critical Nigerian data on HIV-related ocular changes, enriching global research efforts.
Acknowledgments
None.
COMPLIANCE WITH ETHICAL STANDARDS
Conflicts of Interest: The authors declare no competing interests. Financial Disclosure: Nothing to declare. Funding/Support: This work was partly supported by the Fogarty International Center (FIC) and the National Institute on Alcohol Abuse and Alcoholism (NIAAA) of the U.S. National Institutes of Health (NIH) award number 1D43TW011544. The findings and conclusions are those of the authors and do not necessarily represent the official position of the FIC, NIAAA, NIH, the Department of Health and Human Services, or the government of the United States of America. Ethics Approval: Ethical approval was obtained from the local Institutional Research Ethics Committee with approval number NHREC/28/01/2020/EC/3077 on 28th June 2021. Declaration of Participant Consent: Written informed consent was obtained from all participants. Use of Artificial Intelligence (AI)-Assisted Technology for Manuscript Preparation: The authors confirm that there was no use of Artificial Intelligence (AI)-Assisted Technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI. Disclaimer: None.
REFERENCES
- Drug-induced uveitis in HIV patients with ocular opportunistic infections. Ocul Immunol Inflamm. 2020;28((7)):1069-75.
- [CrossRef] [PubMed] [Google Scholar]
- Ophthalmologic Disease in HIV infection: recent changes in pathophysiology and treatment. Curr Infect Dis Rep. 2017;19((12)):47.
- [CrossRef] [PubMed] [Google Scholar]
- Efavirenz-associated retinal toxicity presenting with night vision defects in patients with human immuno-deficiency virus. Ocul Immunol Inflamm. 2020;28((7)):1076-84.
- [CrossRef] [PubMed] [Google Scholar]
- High-resolution ultrasound imaging of the eye – A review. Clin Exp Ophthalmol. 2009;37((1)):54-67.
- [CrossRef] [PubMed] [Google Scholar]
- Ophthalmic artery resistance index is increased in HIV-infected patients and is influenced by Protease Inhibitors Exposure. J Infect. 2014;68((5)):500-3.
- [CrossRef] [PubMed] [Google Scholar]
- Utility and effectiveness of orbito-ocular B-scan ultrasonography in an African developing country. J Health Care Poor Underserved. 2013;24((4)):1440-7.
- [Google Scholar]
- Sampling techniques & determination of sample size in applied statistics research: An overview. Int J Econ Commer Manag. 2014;2((11)):1-22.
- [Google Scholar]
- Comparison of intima-media thickness and ophthalmic artery resistance index for assessing subclinical atherosclerosis in HIV-1 infected patients. Cardiovasc Ultrasound. 2011;9:9.
- [Google Scholar]
- Ophthalmic artery and central retinal artery Doppler patterns in primary open angle glaucoma patients at the Lagos University Teaching hospital, Nigeria. J West Afr Coll Surg. 2018;8((3)):1-21.
- [PubMed] [Google Scholar]
- Usefulness of color doppler imaging of orbital arteries in young hypertensive patients. Proc (Bayl Univ Med Cent). 2019;32((4)):514-9.
- [CrossRef] [PubMed] [Google Scholar]
- High resolution ultrasound with Doppler: A diagnostic adjunct in orbital and ocular lesions in children. Pediatr Radiol. 1992;22:174-8.
- [Google Scholar]
- The orbital contents. In:. In: Anatomy for diagnostic imaging (3rd Ed.). 2010. p. :24-8.
- [Google Scholar]
- Ocular blood flow velocity in primary open angle glaucoma—A tropical African population study. Middle East Afr J Ophthalmol. 2013;20((2)):174-8.
- [CrossRef] [PubMed] [Google Scholar]
- The Basics: Direct and indirect fundoscopy. In:. In: Fundoscopy made easy.. Churchill Livingstone Elsevier; 2010. p. :1-9.
- [Google Scholar]
- Socio-demographic and clinical profile of HIV/AIDS Patients in HAART era at a tertiary care hospital in North-West Rajasthan, India. Int J Community Med Public Health. 2016;3((8)):2088-209.
- [Google Scholar]
- Predictive effects of body mass index on immune reconstitution among HIV-infected HAART users in China. Bmc Infect Dis. 2019;19((1)):373.
- [Google Scholar]
- Ocular manifestations in patients attending antiretroviral therapy centre at a tertiary care hospital in Himachal Pradesh, India. Indian J Med Res. 2018;147((5)):496-500.
- [Google Scholar]
- Relationship between opacity of cytomegalovirus retinitis lesion borders and severity of immunodeficiency among people with AIDS. Invest Ophthalmol Vis Sci. 2019;60((6)):1853-62.
- [CrossRef] [PubMed] [Google Scholar]
- Correlation of CD4 count and severity of dry eye in human immunodeficiency virus positive patients. Int J Sci Study. 2015;3((5)):68-71.
- [CrossRef] [Google Scholar]
- Ocular complications in HIV positive patients on antiretroviral therapy in Ghana. Bmc Ophthalmol. 2016;16((1)):134.
- [CrossRef] [PubMed] [Google Scholar]
- Ocular diseases in HIV-positive patients in a tertiary hospital in Nigeria. World. 2019;13((14)):15.
- [Google Scholar]
- Ocularhaemodynamics parameters of asymptomatic HAART experienced HIV-infected under-five children. Niger J Paediatr. 2016;43((1)):20.
- [Google Scholar]
- Ocular blood flow in patients infected with human immunodeficiency virus. Am J Ophthalmol. 2001;132((5)):720-6.
- [CrossRef] [PubMed] [Google Scholar]



