

Translate this page into:
Can the Internal Nasal Valves Method Be a Game Changer for Preventing Respiratory Tract Infections?

*Corresponding author: Ashok B. Varma, Lakeshore Drive, Fairfield, California, United States. Tel: (+614) 332-9900 ashvarma43220@yahoo.com
-
Received: ,
Accepted: ,
How to cite this article: Varma AB. Can the Internal Nasal Valves Method Be a Game Changer for Preventing Respiratory Tract Infections? Int J Transl Med Res Public Health. 2024;8:e006. doi: 10.25259/IJTMRPH_12_2024
Abstract
An anaphylactic reaction to the influenza vaccine prompted a search for a non-pharmacological way to prevent respiratory tract infections (RTIs) using the internal nasal valves and the innate immune system. The anatomy and physics of the internal nasal valves, using Bernoulli’s principle, can produce a Venturi effect and suction out the pathogen-laden secretions of the nasal cavities, sinuses, nasolacrimal ducts, and Eustachian tubes. The very effective innate immune system could then neutralize these pathogens.
This self-experimentation describes The Internal Nasal Valves (INVals) Method developed by the author for RTIs’ prevention in 1979 and its regular practice since with full compliance and discipline. The coronavirus disease 2019 (COVID-19) pandemic provided him with an opportunity for self-experimentation to perform a trial of The INVals Method on himself despite his age of 73 years and the possibility of highly adverse outcomes.
The author observed, enjoyed, and was impressed with the benefits of The INVals Method during the peak of the COVID-19 pandemic. As of this writing, he has not suffered from any RTIs since using The INVals Method in 1979.
The author’s experiment is a real-world experiment and suggests that The INVals Method may help prevent RTIs and be an ally and complement to the vaccines. Further investigations to test, retest, and test more of the author’s experiment with rigorous randomized controlled trials (RCTs)/cohort RCTs/cluster randomized trials are warranted to support his results. If future research proves that the author’s results are correct and meaningful, it may have a broader clinical impact across medicine as an ally of vaccines, especially in the developing countries where there can be lag period in acquisition and administration of vaccines.
Keywords
Vaccine Ally
RTIs Prevention
Internal Nasal Valves
Venturi Effect
Mucociliary Clearance
Innate Immunology
Gut Immunology

INTRODUCTION
Background of the Study
Respiratory tract infections (RTIs) are a critical ongoing health challenge. The morbidities and mortalities associated with RTIs are severe. Several tools are used to combat these, including pharmacological interventions like the effective life-saving vaccines and non-pharmacological interventions like facial masking, social distancing, and hand hygiene. Regardless of these interventions, concerns about new cases and the long-haul effects they cause keep accelerating. There is a need for more complementary methods for a multipronged, preemptive strike mode on viruses, bacteria, and fungi, which are ubiquitous in the planetary atmosphere.
Acute RTIs claim more than four million lives and cause millions of hospitalizations yearly.[1] According to the World Health Organization (WHO), even before COVID-19, upper RTIs that spread to the lower respiratory tract were the single greatest killer among communicable diseases.[2] In the United States, RTIs account for 37.3% of all hospitalizations, far exceeding that for any other condition.[3] The U.S. Centers for Disease Control and Prevention (CDC) estimates that influenza has resulted in 9–41 million illnesses, 140,000–710,000 hospitalizations, and 12,000–52,000 deaths annually from 2010 to 2020.[4] The annual economic burden is enormous. Although hospitalization costs are important contributors, mortality and lost productivity from missed workdays comprise the bulk of the economic burden of influenza.[5]
Objectives of the Study
Vaccination provides the best protection against preventable respiratory diseases. The most common viruses responsible for respiratory infections are more than 200 different viruses of “common cold,” rhinoviruses, respiratory syncytial virus, influenza viruses, human parainfluenza virus, and human metapneumovirus. However, despite the morbidities and mortalities associated with these viruses, approved and licensed vaccines from the U.S. Food and Drug Administration (FDA) are only currently available for the general population for influenza and RSV viruses.[6] Furthermore, controlling influenza remains a challenge that requires new vaccines each flu season. Researchers and vaccine manufacturers have been working on producing the most effective vaccines possible, but no vaccine is 100% effective. According to the CDC, when flu vaccine viruses are similar and in good agreement with circulating flu viruses, flu vaccination reduces the risk of disease by 40%–60% among the general population.[7] The flu vaccine’s effectiveness varies by type or subtype of influenza virus. Also, certain patients, such as the elderly, immunocompromised, and those with coexisting comorbidities, have weak immune responses to vaccination. Hence, with life-saving vaccines, additional complementary and integrative measures for prevention of RTIs warrant investigation.
Specific Aims and Hypothesis
From childhood into adulthood, the author suffered from influenza, common cold viruses and coinfections, getting on an average two to four infections per year, mostly between September and May (young children suffer from an average of six to eight colds per year, as colds are highly contagious). Nearly all cases involved his lower respiratory tract, causing severe bronchospasm and associated comorbidities lasting several weeks. In the author’s case, all of these were the cause of severe physical and mental anguish and absenteeism from school and work. At age 30, in June of 1979, he had an anaphylactic reaction to his first influenza vaccine (the inactivated whole virus vaccine). His healthcare team told him that his heart rate slowed to single digits, and he received epinephrine and cardiopulmonary resuscitation with endotracheal intubation. He was admitted to Mount Sinai Medical Center, New York University, and received multiple tests, including a thorough neurological exam by a neurologist.
After the anaphylactic reaction in 1979, while rotating through the ear, nose, and throat (ENT) operating room, the author discovered that since the internal nasal valves are the narrowest part of the nasal cavities, they must produce the Venturi effect, which, in turn, must produce a negative pressure in the area of the turbinates, which, in turn, must suck out the pathogen-laden secretions out of the sinuses, the nasolacrimal ducts, and the Eustachian tubes. These pathogens can then be neutralized by the innate immune system and the hostile environment of the stomach. Using this knowledge, the author developed The INVals Method, which may add to our current repertoire as an ally of vaccines.
METHODS
Demographics
Gender: Male. Year of birth: 1949. Occupation: Retired Physician, San Francisco Bay Area, U.S.A. Level of Education: Fellowship in Medicine (Highest level of Education in the field of Clinical Medicine in the United States). Weight: 56.2 Kgs (124 lbs.). Height: 1.74 m (five feet nine inches). History of Medical (Physical and Mental) Conditions: None. Family history: Paternal side—severe proneness to influenza and other common cold viruses. Maternal side—moderate proneness to influenza and other common cold viruses.
Part 1, Pre-1979 (i.e., When No Influenza Vaccines were Administered to the Author)
Age 0–30 years old—Period of 30 years
Because of lack of awareness, there was no administration of any influenza vaccines during this time period. Thus, the author served as his own control from birth to the age of 30 years when he suffered from repeated RTIs every year.
Part 2, Post-1979 (Devising The INVals Method)
The author devised The INVals Method after the anaphylactic reaction to the influenza vaccine. In order to prevent hyperventilation, he incorporated The INVals Method with exercise. The INVals Method is very well demonstrated in the YouTube video: https://youtu.be/POVW9QA-HEc. He almost always performed The INVals Method whenever he felt a cue that a cough or sneeze was about to come, thus helping clear the source of irritation and help prevent the transmission of pathogens to others. It was of importance to do The INVals Method on an empty stomach in the morning and an almost empty stomach before going to bed; thus, he avoided the dilutional effect from ingested food which causes reduced stomach acidity.
DATA COLLECTION AND TESTS PERFORMED
Additional Testing
In addition, there was thorough screening of the author’s donated blood by the American Red Cross (Washington, DC, U.S.A.) and Vitalant Blood Donation (Vitalant Blood Donation, Phoenix, Arizona, U.S.A.) once every three months. The donated blood was tested for viral RNA, Hepatitis B, Hepatitis C, and blood cultures for any Infectious agents. (Creative Testing Solutions, Phoenix, Arizona, U.S.A.).
Part 3, COVID-19 Pandemic
During the COVID-19 pandemic, the author consulted with his primary care physician regarding the COVID-19 vaccine, and due to his severe anaphylactic reaction in 1979, he was ordered not to use it. Therefore, the author did not receive a COVID-19 vaccine and used The INVals Method during the period of the COVID-19 pandemic.
Prospective Challenge Study
The Prospective Challenge Study was done to test the author’s concept during the explosive and peak period of the COVID-19 pandemic from January 2 to September 1, 2021, for a total of eight months.
Age: 72–73 years old.
Setting: California, Nevada, Arizona, New Mexico, Texas, and Oklahoma. (All in the United States. Arizona, Texas, and Oklahoma were intentionally chosen because there was no mandatory facial masking or social distancing, and all indoor gatherings were allowed.)
Exposure to COVID-19 Virus
During this period, the author intentionally stayed in motels and hotels converted into homeless shelters, where most residents were noncompliant with public health guidelines and seldom observed facial masking, social distancing, and hand hygiene. Ventilation in these facilities was questionable, and the windows were locked shut for the residents’ safety. For purposeful exposure, he spent the evenings in Las Vegas or Native American casinos in all the states mentioned above, where smoking and alcohol consumption are allowed 24 hours per day, seven days per week, and no social distancing was observed. During the day, much time was spent indoors at art museums, natural history museums, and indoor superspreader events. The most precise, accurate, and intense exposure measures were used in all real-world environments.
The INVals Method was performed daily and immediately after exposure to crowds, travel, and gatherings. Whenever a motel or hotel was overcrowded indoors, he preferred to do The INVals Method outdoors.
Predominant COVID-19 Viruses
During this period of the Prospective Challenge Study, according to WHO, the predominant COVID-19 variants with very high risk of transmissibility, hospitalization, and mortality were as follows[8]:
COVID-19 Alpha Variant: December 18, 2020
COVID-19 Beta Variant: January 14, 2021
COVID-19 Gamma Variant: January 15, 2021
COVID-19 Delta Variant: May 21, 2021
Data Collection and Tests Performed During COVID-19 Part of the Study
Genome Sequencing
Genome sequencing and DNA Screening were performed to eliminate any confounding biases for any immunologically related gene variants, for any potential health predispositions, for any evidence of DNA sequence mutation by way of infections by viruses, and for genetic variants on genetic results of more than 2700 genetic markers, including those of the immune system (FDA approved 23 and Me, Sunnyvale, California, U.S.).
Diary Recording
The INVals Method Diary: The following were done and recorded on a daily basis: Symptoms and signs of COVID-19 infection, including Temperature, Heart rate, Respiratory rate, Blood Pressure, Blood Oxygen Saturation (SpO2), and Weight.
Blood Tests
Annual immunologic tests were done, as shown in Table 1.
| Test | Results Range | Additional Information |
|---|---|---|
| Complete Blood Count | 4.5–5.6 thousand/µL | Leukocytes are the body protectors. Each of the five varieties of leukocytes play its own specific role in defending the body against infections and illness. |
| Absolute Lymphocytes Count | 783–917 cells/µL | Since ALC were always within reference range, it was not necessary to conduct T-cell count, natural killer cell count, B-cell count, and lymphocytes subsets analysis. Since there were no symptoms and signs of COVID-19 and the results for absolute lymphocytes counts, immunoglobulin levels, and biomarkers for inflammatory responses were within the reference range from January 2, 2021, to September 1, 2021, it was not necessary to perform lymphocyte subpopulations of CD3, CD4, CD8, and CD19. |
| Immunoglobulin Levels | 2.0–3.1 g/dL | Since there were no symptoms and signs of COVID-19 and the results for immunoglobulin levels were always within reference range, it was not necessary to conduct separate tests for IgA, IgM, and IgG. |
| Thyroid Function Tests | TFTs were conducted as thyroid hormone may act as a modulator of immune activities at the cellular level. | |
| T4 Free | 1.6–1.4 ng/dL | |
| Thyrotropin | 3.04–3.16 mlU/L | |
| Liver Function Tests | LFTs were conducted as the liver is also a key frontline innate immune system organ, ideally positioned to secrete bile and IgA antibodies which capture and clear viruses, bacteria, and other pathogens entering the body through the gastrointestinal tract. | |
| Alkaline Phosphatase | 56–88 U/L | |
| ALT | 11–27 U/L | |
| Total Bilirubin | 0.8–0.9 mg/dL | |
| AST | 17–21 U/L | |
| Renal Function Tests | Kidney disease affects general immunity causing intestinal barrier dysfunction, systemic inflammation, and immunodeficiency that contributes to morbidity and mortality in patients. | |
| Creatinine | 1.09–1.1 mg/dL | |
| Serum Urea Nitrogen | 20–22 mg/dL | |
| Serum Ferritin Levels | 13–36 ng/mL | Ferritin levels were done to identify inflammatory markers as ferritin is elevated in its capacity as an inflammatory marker. |
COVID-19: Coronavirus disease 2019, ALC: Absolute lymphocytes count, Ig: Immunoglobulin, TFTs: Thyroid function tests, LFTs: Liver function tests, ALT: Alkaline aminotransferase, AST: Aspartate aminotransferase.
All tests were performed by Quest Diagnostics (Secaucus, New Jersey, U.S.A.).
Blood Serology Testing for COVID-19 Antibodies and Other Pathogens
Thorough screening of my donated blood to Vitalant Blood Donation (Vitalant Blood Donation, Phoenix, Arizona, U.S.A.) was done once every three months. The donated blood was tested for COVID-19 antibodies, viral RNA, Hepatitis B, Hepatitis C, and blood cultures for any infectious agents (Creative Testing Solutions, Phoenix, Arizona, U.S.A.).
Polymerase Chain Reaction Testing
The COVID-19 testing included SARS-COV-2 RNA, QL NAAT, RT Polymerase Chain Reaction (PCR)/TMA Tests were performed every two months (Laboratory Corporation of America, Burlington, North Carolina, U.S.A.), and Rapid COVID-19 Antigen Self-tests (BinaxNOW, Abbott Diagnostics, Scarborough, Maine, U.S.A.) were performed twice a week on Tuesdays and Fridays, from the day they were introduced into the market (April 19, 2021).Since studies proved that the incidence of false results with rapid antigen self-tests were relatively high, testing with gold standard RTq PCR tests and blood serology tests for COVID-19 antibodies were also continued.[9]
RESULTS
Part 1, Pre-1979 (i.e., When No Influenza Vaccines were Administered to the Author)
The author identified all the severe morbidities he was suffering from before 1979. They were two to four influenza and cold viruses infections every year.
Part 2, Post-1979 (Period After the Anaphylactic Shock to Influenza Vaccine)
Retrospective Challenge Study. Age 30–75 years old. Period of 45 years. After the anaphylactic reaction to the influenza vaccine in 1979, the author using his educational background devised The INVals Method. The results of this Method have been that the author had no influenza, no RTIs, and had 100% work attendance since 1979.
Results of Blood Tests
The tests shown in Table 1 were done every year and the results were all within normal limits.
Results of Advanced Blood Tests
Screening tests performed on donated blood every three months showed the following: Hepatitis B—negative; Hepatitis C—negative; human T-lymphocytic virus (HTLV)—negative; viral RNA—negative; cytomegalovirus—negative; and blood cultures for any infectious agents—negative.
The performance of all the above tests on donated blood was relevant in how they affect the human immune system. Health screenings at the American Red Cross and Vitalant Blood Donations once every three months were always within normal limits.
Part 3, COVID-19 Pandemic
Following are the results of Part 3, COVID-19 pandemic Prospective Challenge Study:
Results of Diary Maintenance
The record entered in the diary during this period on a daily basis : Symptoms of COVID-19—none were present during the whole duration of this Prospective Challenge Study.
Signs of COVID-19—none were present during this period.
Vital signs: Temperature, Blood Oxygen Saturation (SpO2), Heart Rate, Respiratory Rate, Blood Pressure, and Weight were all within normal limits during this period.
Genome Sequencing and DNA Screenings Analysis Study
No gene variants associated with the immune system were detected. No new disease genes were discovered. No immunologic, respiratory, or hematologic disorders were discovered on genome sequencing. No potential health predispositions were detected. There was no evidence of DNA sequence mutation by way of infection by viruses. The genetic variant reports based on genetic results of more than 2700 genetic markers, including those of the immune system, were negative.
Laboratory Blood Studies
The results are shown in Table 1 and were within normal range.
Results of PCR Testing
Quantitative reverse transcription PCR (RT-qPCR) tests were performed every two months starting from January 2021. The author continued performing the PCR tests every two months in spite of the availability and performance of rapid antigen tests for COVID-19, which were made available on the market on April 19, 2021. The results for all the PCR Tests for COVID-19 were negative during this period.
Results of Rapid Antigen Tests
The tests were performed twice a week—every Tuesday and Friday. The results of all these tests were negative for the whole duration of this period.
Results of Serology Tests for COVID-19 Antibodies
These tests were performed every quarter (three months) on donated blood. No COVID-19 antibodies were detected anytime during the whole duration of this period. Serology tests on donated blood were also performed every quarter for the immune system-related pathologies for viral RNA, Hepatitis B, Hepatitis C, human T-lymphotropic virus, and cytomegalovirus; they were all negative. Blood cultures for any infectious agents were negative.
Current Status
The author continues to challenge and test The INVals Method by attending events that draw attendees worldwide, such as Rotary International and the New Year’s Eve celebration in Times Square, New York City, which gathers people worldwide in a shoulder-to-shoulder environment. The results of ongoing twice-weekly rapid antigen tests and blood serology tests remain negative as of this writing in April 2024.
DISCUSSION
Discussion of the Results
The author’s study, which has three parts, shows the results over a period of 75 years.
Results of the First Part (i.e., When No Influenza Vaccines were Administered to the Author)
The results of the First Part (0–30 years) are clear, with the author’s afflictions, torments, and misery with the RTIs.
Second Part (Period After the Anaphylactic Reaction to Influenza Vaccine)
After his anaphylactic reaction to the influenza vaccine in 1979, by asking how things can be done more quickly and more easily because when it comes to the innate immune system, timing is everything, the author devised The INVals Method. He fully used the basic fundamental anatomy and physics of the internal nasal valves (which produce the Venturi effect), the nasal cavities, the sinuses, the nasolacrimal ducts, the Eustachian tubes, and the nasopharynx to develop The INVals Method to free himself from the RTIs of the first 30 years of his life. He had results that freed him from the RTIs and their severe associated morbidities.
Third Part (COVID-19 Pandemic)
To eliminate the factor of random errors as a result of the operation of chances or any biases in the use of The INVals Method, the author used the opportunity of performing the Prospective Challenge Study during the explosive and peak period of the COVID-19 pandemic exposing himself to massive life-risking dosages of the virus. These results may highlight opportunities for decreasing human vulnerabilities to new emerging and evolving respiratory pathogens.
The results of parts 2 and 3, extending over the period of 45 years, showed the usefulness and simplicity of The INVals Method, which is minimalist, yet in the author’s experiment, very effectively prevented viral and bacterial respiratory infections.
Internal Nasal Valves, Bernoulli’s Principle, and the Venturi Effect
In practical terms, the Venturi effect directly corresponds to Bernoulli’s principle. The internal nasal valves constrict streamlined airflow, as shown in Figures 1, 2, and 3, increasing the velocity of inhaled air and decreasing pressure, creating a partial vacuum to suction out secretions from the sinuses, nasolacrimal ducts, nasopharynx, and Eustachian tubes.[10] In Figure 3, the airflow in “1” (i.e., the areas below the internal nasal valves) is lower than the airflow in “2” (i.e., the areas of the internal nasal valves). Because the cross-sectional area at “1” is greater than at “2”, this creates the Venturi effect where the formula is: p1-p2 = P/2(v2/2-v2/1).
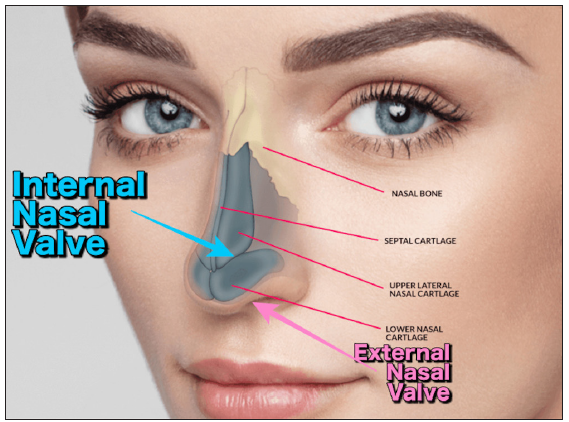
- Internal nasal valve anatomy.
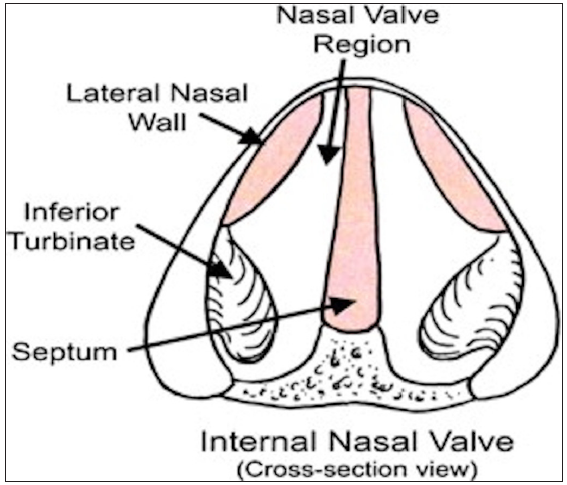
- Cross-section of the internal nasal valves.
![Diagram illustrating the Venturi effect. A1: External nasal valve, A2: Internal nasal valve, 1: Nasal cavity below the INV, 2: Area around the INV, ∆h: Height of the nasal cavity, h: Height of the paranasal sinuses, P1, P2: Pressure at position, P: Density of air, v1: Slower air velocity where nasal cavity was wider, v2: Faster air velocity where internal nasal valves are narrowest part of air passage. This Venturi effect suctions out particulate-laden mucus from the nasal cavities, sinuses, nasolacrimal ducts, and Eustachian tubes. (Image Credit: Diagram illustrating the Venturi effect (https://commons.wikimedia.org/wiki/File:Venturi5.svg] by HappyApple, 2003. Public Domain).](/content/160/2024/8/1/img/IJTMRPH-8-e006-g3.png)
- Diagram illustrating the Venturi effect. A1: External nasal valve, A2: Internal nasal valve, 1: Nasal cavity below the INV, 2: Area around the INV, ∆h: Height of the nasal cavity, h: Height of the paranasal sinuses, P1, P2: Pressure at position, P: Density of air, v1: Slower air velocity where nasal cavity was wider, v2: Faster air velocity where internal nasal valves are narrowest part of air passage. This Venturi effect suctions out particulate-laden mucus from the nasal cavities, sinuses, nasolacrimal ducts, and Eustachian tubes. (Image Credit: Diagram illustrating the Venturi effect (https://commons.wikimedia.org/wiki/File:Venturi5.svg] by HappyApple, 2003. Public Domain).
In the internal nasal valves, the airway size decreases dramatically, creating the narrowest areas of the nasal cavities which account for the resistance to respiratory airflow. The author came up with the concept that by using Bernoulli’s principle, the Venturi effect is created, which suctions out the foreign particle-laden secretions from the areas of the nasal cavities, the sinuses, the nasolacrimal ducts, and the Eustachian tubes. (Adapted from Rinoplasti (https://commons.wikimedia.org/wiki/File:Rinoplasti.png) by Ozan Balik, licensed under the Creative Commons Attribution-Share Alike 4.0 International license). Internal and external nasal valve labels and arrows were added.
The narrowest part of the nasal cavity is the internal nasal valves located between the septum and the inferior turbinate, which creates the Venturi effect using Bernoulli’s principle. Image credit: Rhee JS, Weaver EM, Park SS, Baker SR, Hilger PA, Kriet JD, Murakami C, Senior BA, Rosenfeld RM, DiVittorio D. Clinical consensus statement: Diagnosis and management of nasal valve compromise. Otolaryngol Head Neck Surg. 2010;143(1):48–59. DOI:10.1016/j.otohns.2010.04.019. © 2010 SAGE Publications. Used with permission.
Bernoulli’s Equation and Venturi Effect: Cambridge University Press: 05 July 2014. ET Gilbert and MD Wittenberg. It is on the physics of this Venturi effect that the home vacuum cleaners work by creating negative pressure inside the machine.[11]
In real life, when performing The INVals Method, one can see the nasal nares puckering in, the feeling of the internal ears being pulled into the center of the head, and when the eyes are welled up with tears, the tears getting sucked into the nasal cavities. All of this is because of the negative pressure created by the Venturi effect. These two “Venturi pumps” are air-powered and placed close to the sinus openings in the turbinates for fast response and minimal vacuum loss. No moving parts ensure long life with low maintenance. Since they are air-powered, they do not require an electrical power source or lubricant; hence, the vacuum is clean and efficient.
Nasal Cavities
Nasal cavities are the first defense against pathogens, allergens, and toxins. Depending on size, a human secretes 1–1.5 L of upper respiratory tract secretions daily.[12] The pH of these secretions is acidic, between 5.5 and 6.5. The primary function of these secretions is to trap the pathogens, allergens, and pollutants ubiquitous in the planetary environment. An adult human breathes 7000–11,000 L of air per day. In addition to air, 10,000–1,000,000 pathogens are inhaled per cubic meter.[13] The mucociliary clearance is important for airway protection. The most important fact about the mucociliary clearance is that the cilia beat in a metachronous and coordinated fashion that results in waves that travel across the epithelium propelling the trapped pathogens. The direction of the mucociliary waves is targeted toward the inlet of the esophagus, upwards from the lower respiratory tract, and downwards from the upper respiratory tract. Thus, The INVals Method can effectively promote this directional movement by creating negative pressure and suctioning out the pathogen-laden secretions which are periodically deglutated subconsciously. The ciliary beat frequency is decreased by low temperatures, acidification, and air pollutants. Also, during cold ambient temperatures, the extra-cellular vesicles which are important for nasal immunity decrease significantly. Hence, here The INVals Method can be helpful.
The streamlined airflow through the internal nasal valves help the mucus layer mediate clearance of virtually all inhaled pathogens in the nasal cavities, sinuses, nasolacrimal ducts, and the Eustachian tubes. Mucociliary clearance draws mucus away from the middle ear into the nasopharynx, thus preventing infection from ascending into the middle ear. Viruses, bacteria, fungi, and allergens captured by mucus are transported by mucociliary clearance to the nasopharynx at 1 cm per minute.[14] The pathogen-laden mucus is deglutated subconsciously and replaced every 10–20 minutes.[15] Therefore, humans deglutate mucus all day without knowing it. Most droplets in the air are filtered in the nasal cavities or deposited in the sinuses, nasopharynx, and oropharynx. The mucus in the trachea catches small droplets and expels them into the oropharynx where they are subconsciously deglutated. The constant clearance of mucus toward the esophagus is the most important preventive mechanism.[16] Thus, vigorous inspiration using The INVals Method can create a marked negative pressure in the nasal cavities and can allow for quicker transportation of these secretions with captured pathogens, pollens, and toxins toward the esophagus. Gastric secretions will quickly neutralize pathogens within the mucus.
Inhalation is the most common route for pathogens to enter the human body. Pathogen entry factors are expressed at high levels in nasal and sinus epithelial cells. Respiratory infectious agents use the nasal port to enter a new host, and the target cells are right at the portal of entry. Fortunately, the upper respiratory tract is well equipped to prevent these pathogens from causing pathological conditions. Secondary lymphoid organs are present in the mucosal tissues, such as nasal-associated lymphoid tissue, mucosal-associated lymphoid tissue, adenoids, tonsils, and lymphoid follicles. By stimulating innate immune system receptors, these host defense pathways are critical therapeutic strategic processes to prevent diseases. Innate immune system interactions in the mucosa are complex and tightly regulated to maintain a healthy inflammatory tone and distinguish between a healthy microbiome from pathogenic organisms. Innate immune receptors important for prevention of diseases from pathogens include toll-like receptors, nod-like receptors, and C-type lectin receptors. These receptors regulate the secretion of cytokines and chemokines and the conditioning of immune cells for direct antimicrobial activity. Furthermore, epithelial cells form a single layer with tight junctions that restrict pathogens from accessing the host. The pathogens trapped in the mucus around the target cells at the portal of entry in the nasal cavities, nasal lacrimal ducts, sinuses, and Eustachian tubes can be sucked out by the negative pressure created by the Ventui effect of The INVals Method and on deglutition are neutralized by the gastric secretions.
Immunoglobulin A, Antimicrobial Peptides, Nitric Oxide, Microbiome, and Secretory Immunoglobulin A in the Upper Respiratory Tract
Large amounts of immunoglobulin A (IgA) are synthesized by mucosal sites in the upper respiratory tract. IgA can act at the very beginning of an infection when the number of pathogens is low. This has significant consequences since fighting the pathogens is a numbers game. A loss in the battle against pathogens is unlikely to occur during the replication of a few pathogens, but the chances increase as more pathogens are present. Hence, the importance of doing The INVals Method at appropriate intervals, which also ensures a streamlined flow of air through the internal nasal valves and keeps the Venturi effect at its peak performance. Once infection, inflammation, and increased mucus secretions set in, they create uneven surfaces in the areas of the internal nasal valves and can adversely affect Bernoulli’s principle and the Venturi effect.
The human immune system has ingenious methods to attack pathogens at the portal of entry. The innate immune system is responsible for dealing with most infections from pathogens in the upper respiratory tract. The respiratory surface epithelium secretes more than 100 antimicrobial peptides (AMPs) such as lysozyme, lactoferrin, defensins, and reactive oxygen species (ROS) such as hydrogen peroxide and nitric oxide.[17] Nitric oxide directly increases mucociliary clearance. In addition, the upper respiratory tract microbiome can affect the outcome of infections by modulating the innate immune system and gene expression. The upper respiratory probiotic microbiome produces antimicrobials and inhibits pathogens’ growth by changing the pH. In addition, these probiotic bacteria have various other positive immunomodulatory functions.[18]
Nitric oxide in the upper respiratory tract is a known antimicrobial agent. AMPs (e.g., defensins) are part of an innate immune response found in neutrophils in the sinuses and nasal cavities and kill bacteria, fungi, and certain viruses. Macrophages and monocytes are highly phagocytic for pathogens. The lamina propria, located beneath the epithelium of the respiratory and gastrointestinal tract, is populated by tissue whose key function is the secretion of IgA antibodies into the lumen. The lamina propria also contains macrophages, dendritic cells, mast cells, eosinophils, and neutrophils. Secretory IgA (sIgA) is derived from locally produced IgA. Its main function is to neutralize foreign substances and prevent systemic access. The naïve total human antibody repertoire could easily comprise as many as one quintillion—a million trillion—unique antibodies.[19] Hence, unlike the case with antivirals and antibiotics, where the continuously evolving variants develop resistance, the human immune system practically never runs out of effective measures to tackle these variants. Enveloped viruses have the capacity of cell-cell transmission, infecting neighboring cells without being released to the outside of the cells; thus, the viruses associated with these cells are physically protected from neutralizing antibodies.[20] This mechanism likely causes a delay in detection by the immune system. Therefore, it is important to denature these viruses right at the portal of entry, and The INVals Method helps in suctioning out the pathogens from the sinuses, nasolacrimal ducts, nasopharyngeal area, and the Eustachian tubes and exposes them to mechanisms of denaturing them and deglutating them into the very hostile environment of the gastrointestinal tract.
Nose Blowing
Nose blowing causes a marked increase in intranasal pressure and causes the pathogens in the nasal cavities to be propelled into the remote areas of sinuses, nasolacrimal ducts, and the Eustachian tubes. This causes inflammation in these areas that hampers the mucociliary mechanisms and prevents pathogens from being swept out.[21] This also promotes the formation of biofilms in the sinuses.[22] Good nasal hygiene and etiquette are essential to preventing infections and disease transmission to others. A cultural taboo toward nasal, sinuses, nasolacrimal ducts, and Eustachian tubes secretions are modifiable risk behaviors, and awareness that nose blowing is detrimental to one’s health and hygiene and promotes the spread of diseases is very important. To prevent the transmission of infections, efforts must focus on changing behavior and modifying respiratory etiquette culture, a point that The INVals Method emphasizes.
While oral hygiene practices are common in the morning and before bedtime, nasal hygiene is often ignored. Practicing The INVals Method involves excellent nasal hygiene and does not require special equipment. Furthermore, using nasal lavage devices, bulb syringes, and other items can cause micro tears or scratches on the mucous membranes, creating an accessible entry port for microorganisms to access epithelial cells and the bloodstream and causing infections. Worse, such devices can successfully push pathogens deeper into the sinuses and nasolacrimal ducts.
The Sinuses
The sinuses share the same defense mechanisms against pathogens as the nasal cavities. However, sinuses can easily form biofilms. Biofilms are reservoirs for pathogens contained in a polymer-encased protective matrix, making it very difficult to treat. Biofilms are a significant cause of chronic rhinosinusitis infections and may cause systemic inflammation.[22] Prevention is the best cure for biofilms, making good and regular nasal hygiene important. The INVals Method may help in achieving this.
Nasolacrimal Ducts
In the nasolacrimal ducts, the defense mechanisms of the mucosa are the same as those of the nasal cavities. Nose blowing can push nasal secretions up the nasolacrimal ducts and be the source of infection, causing dacryocystitis and other eye infections. The INVals Method may help here in preventing these pathologies.
Eustachian Tubes
In the Eustachian tubes, the defense mechanisms of the mucosa are the same as those of the nasal cavities. Mucociliary clearance drains the mucus from the middle ear into the nasopharynx, preventing infection from ascending into the middle ear. Infections from the upper respiratory tract, including the sinuses, can spread to the Eustachian tubes causing inflammation of the tubes and various clinical conditions, namely acute otitis media, chronic otitis media, and Eustachian tube dysfunction, causing reduced hearing and balancing problems. These are more common in children than adults because children’s Eustachian tubes are shorter and more horizontal. The INVals Method could be easily taught to young children starting from the toddler age, which may help prevent the aforementioned conditions because the negative pressure created sucks out all the pathogens out of the Eustachian tubes and on deglutating causes their neutralization in the very hostile environment of the stomach.
Gastrointestinal Tract
Almost everything mentioned above about the upper respiratory tract and its innate immune system also applies to the gastrointestinal tract and the innate immune system associated with it. However, the following features are unique to the gastrointestinal tract and its innate immune system. Most human microbiomes reside in the gastrointestinal tract, as does 70%–80% of the human body’s immune system.[23] Gastric juice is a unique combination of hydrochloric acid (HCl), pepsin, and lipase. These are found in all vertebrates, and they inactivate deglutated pathogens. Gastric juice, innate immune system antibodies, bile, pancreatic secretions, gastrointestinal microbiome, and innate immune system cells (e.g., natural killer cells, phagocytes like neutrophils, macrophages, mast cells, and dendritic cells) complement each other as a defense against the invading pathogens. Furthermore, the nitrate in saliva and food is converted by Lactobacilli in the mouth into nitrite, which, in the stomach, is transformed by gastric juice into nitric oxide, a robust antimicrobial agent.
Gastric juice has a pH of approximately 1.5 and can kill bacteria and enveloped viruses in approximately 15 minutes if the pH is < 4.0.[24] If the pH is > 4.0, the pathogens can survive. Therefore, it was beneficial for the author to do The INVals Method on an empty stomach in the morning and an almost empty stomach before going to bed, which avoided the dilutional effect of ingested food that causes the stomach pH to rise. However, the pathogens that escape the very hostile environment of the stomach are neutralized by bile salts, which are potent detergents. At other times during the day, the author did The INVals Method about 15 minutes before consuming meals. Interestingly, the physiological apparatus of gastric acid secretion is designed to keep the gastric pH below 4.0, the pH level essential to kill potential microbiological invaders.[25] Pepsin plays a very complementary role with HCl, causing a marked increase in pathogenic susceptibility to proteolysis in killing the pathogens.
The mucus layer of the gastrointestinal tract is very thick. A pathogen traversing the mucus layer is analogous to a human swimming through 150 gel-filled soccer fields.[26] This mucus layer contains sIgA and other secreted factors, such as AMPs that have antipathogenic activity. In addition, there is a beneficial microbiome of the gastrointestinal tract. Epithelial cells of the gastrointestinal tract are also joined by tight junctions barring pathogen entry to the deeper layers.
The liver, part of the gut-liver axis, has a vital role in pathogens in the gut and influences pathogens in the gut via the production and release of bile and IgA antibodies. Bile causes emulsification and solubilization of lipids and affects the phospholipids and proteins of pathogen membranes, thus disrupting pathogen homeostasis.[27] Plasma cells originating in the Payer’s patches colonize the portal regions and the submucosa of the biliary tract and produce IgA antibodies in the liver. This IgA is secreted into the bile and is important for controlling pathogenic loads.
General Discussion
Bacteria, Viruses, Fungi: Cytokine Storm. Long-Term Effects
Bacteria, fungi, and allergens are ubiquitous and require preventive measures to avoid illnesses. A robust immune system will not always protect from the worst aspects of pathogenic infections and could induce a cytokine storm. The cytokine storm killed many healthy young people during the 1918–1920 pandemic and recently during the bird flu and swine flu pandemics.[28] The INVals Method may prevent such critical events from occurring. Preventing the development of infection may decrease the likelihood of health problems from post-infection sequelae, such as long-term COVID-19 or long-term influenza, whose burden extends far beyond the acute phase of the infection. The INVals Method may help prevent these conditions.
Low- and Middle-Income Countries
Low- and middle-income countries lag behind high-income countries in vaccine acquisition and administration and may need allied non-pharmacological interventions for prolonged periods.[29] The INVals Method may act as a complement to other measures like mask use, social distancing, and hand washing during this period. More importantly, The INVals Method may complement and integrate with vaccine use and bolster the immune response in the immunocompromised, the elderly population, and those with existing comorbidities.
Correct Technique for The INVals Method
When performing The INVals Method, exhaling through the mouth when lifting, pushing, and pulling is imperative. It is also very important to inhale vigorously through the nose when releasing. Most exercisers commonly breathe through the mouth, especially as the intensity of the exercise mounts. Inhaling through the nose, which is the best humidifier, is very important because the nose humidifies the dry air to 100% humidity, which is essential for a healthy mucociliary mechanism for the entire respiratory system and it also traps pathogens in the air.[30,31]
Differences Between Aerobic Exercise and The INVals Method
An important question that is raised is whether The INVals Method differs from the standard aerobic exercise. The author engaged in regular aerobic and anaerobic exercises until age 30, but still experienced frequent RTIs. The INVals Method differs from aerobic and anaerobic exercises in several ways:
-
(1)
Avoiding mouth breathing to inhale is crucial, even during intense exercise.[31]
-
(2)
The INVals Method involves inhaling briskly through the nose and exhaling through the mouth, utilizing the Venturi effect created by the internal nasal valves.
-
(3)
The INVals Method is performed first thing in the morning on an empty stomach to eliminate the factor of dilutional effect and to ensure that the lethal environment of the stomach effectively eliminates pathogens collected in the upper respiratory tract during sleep.
-
(4)
The INVals Method is performed almost every four to six hours on a relatively empty stomach approximately 15 minutes before meals (again to avoid the dilutional effect from ingestion of food).
-
(5)
The INVals Method is performed after exposure to crowds or visits to hospitals, nursing homes, or places of social gatherings.
-
(6)
The INVals Method must be performed diligently, daily, without skipping, as pathogens do not take holidays.
-
(7)
The INVals Method can be performed anywhere, even while on the go.
-
(8)
During the performance of The INVals Method, frequently taking very vigorous and deep inspirations followed immediately by deglutating is significant for neutralizing the pathogens. Hence, The INVals Method is very different from aerobic exercise or the well known American Lung Association breathing techniques for chronic obstructive pulmonary disease or the mindful breathing exercises.
Whenever the author performed The INVals Method, he enjoyed involving the whole family when possible. The author set notifications on his smartphone to help remind him of the daily routine of The INVals Method.
Taboo Toward Deglutition of Secretions
It deserves to be emphasized the need to get rid of the taboo around deglutating of secretions. Humans deglutate all day subconsciously deglutating 1–1.5 L, even deglutating them three to four times per hour during sleep—that is about 24–32 times during eight hours of sleep.[32]
The INVals Method and “Exercise Resistance”
A very important benefit of The INVals Method is that it provides a strong incentive for regular short exercise, as short as 45 to 120 seconds, every four to six hours throughout the day. The American College of Sports Medicine considers a vigorous 45 minutes to an hour of exercise in the morning followed by no exercise during the rest of the day as a sedentary lifestyle which can lead to “exercise resistance,” where fat metabolism is more influenced by the inhibitory effects of inactivity than by the stimulating effects of one hour of intense exercise in the morning.[33]
The INVals Method and Position
For the author, the performance of The INVals Method was useful in any position. Bernoulli’s equation is a more general and mathematical form of Bernoulli’s principle that also considers changes in gravitational potential energy and height. The four pairs of sinuses are located in different parts of the skull, at different heights, and connect to the nasal passages in a complex network of drainage passages draining the mucus, which is deglutated subconsciously. Hence, it was helpful but not necessary for the author to perform The INVals Method in different positions.
Best Practice Algorithm for The INVals Method as Followed by the Author
-
1.
First thing in the morning on waking up with an empty stomach perform 30–40 sit-ups in bed that takes 30–40 seconds. If desired, do more and personalize it , see “a” and “c” below.
-
2.
Performing sit-ups or body weight exercise or exercise using equipment like weights before lunch—very important to keep (a) in mind when performing The INVals Method. Use of smartphone alarms are very helpful. If busy with work, set up a timer on smartphone to catch up with The INVals Method later (b, c).
-
3.
Around 3 pm, perform The INVals Method for a period depending on availability of time, but at least for 30–40 seconds—for example, performing sit-ups, lateral sit-ups, dumbbell exercises, and more (a, b, c).
-
4.
In the evening when performing regular exercise, like jogging, power walking, or weight lifting, The INVals Method is incorporated into these by vigorous inhalations through the nose and exhalations through the mouth, thus fully utilizing the Venturi effect created by the internal nasal valves, sucking out all the pathogens trapped in the nasolacrimal ducts, the sinuses, and the Eustachian tubes and sending them to the graveyard in the very hostile environment of the stomach. Involving the whole family is of benefit by catching children, including toddlers, at an early age to imprint good habits into them (a, b, c).
-
5.
Before going to bed, perform 30–40 sit-ups (or some variations of these). If desired, do more and personalize (a, b, c). Hence, the effort and time associated with The INVals Method encourage its utilization.
-
a.
Very important to breathe out through the mouth and vigorously breathe in through the nose, thus fully using the Venturi effect produced using the Bernoulli’s principle. At the end of The INVals Method, take an extra vigorous deep inhalation through the nose and swallow.
-
b.
This fulfills the recommendation of American College of Sports Medicine which considers that a vigorous 45 minutes to an hour of exercise in the morning followed by no exercise during the rest of the day as a sedentary lifestyle leading to “exercise resistance.”[33]
-
c.
The INVals Method has to be done seven days a week, including when on vacation as pathogens take no holidays or vacations. Can be done anywhere—on a beach, park bench, you name it.
-
Protocols that May Help for Future Replication of Research
Future research is warranted to test The INVals Method in standardized, unbiased RCTs/cohort RCTs/cluster randomized trials before The INVals Method’s results can be generalized. The protocol developed by researchers for hand hygiene and facial masking and published in medical journals might be modified to conduct robust RCTs/cohort RCTs/cluster randomized trials.[34–36] It is of utmost importance to have more effective complimentary tools in our toolbox to tackle future pandemics and epidemics.[37,38]
DNA analysis and genome studies excluded any confounding biases, nonmeaningful measures, and erroneous assumptions.[39] This test may not be essential for RCTs in the general population.
Strengths
The author’s experience spans 75 years, including during the COVID-19 pandemic. Despite being aware of the risks of severe morbidity and mortality, the author undertook the self-experimentation with The INVals Method during the pandemic. This self-experimentation may prove that The INVals Method is a strong vaccine ally. Its strength is in its simplicity and zero cost with positive side effects and no harm.
Limitations
A thorough search of PubMed, the Cochrane Library, Google Scholar, and Science Direct for previous publications, case reports, and studies yielded no similar studies against which to compare the author’s self-experimentation design or results. Given his pre-1979 RTIs frequency, he had to invent The INVals Method because of the lack of suitable alternative treatments. This is the first self-experimentation to experiment the use of the author’s novel method for preventing his RTIs, which incorporates the role of the internal nasal valves, Bernoulli’s principle creating the Venturi effect, the role of the innate immune system, and the gastrointestinal tract.
This is a self-experimentation with an N-of-one because the author did not want to use other persons as experimental candidates. Self-experimentations are important as discoveries are not made by committees or group of workers; they originate in the minds of single individuals. There is no important discovery in medicine in the last more than 100 years that evolved out of group research; the ideas of discovery are still going to come from the idea in one individual’s mind. Scientists say that self-experiments must be allowed to make progress on intractable problems.[40]
CONCLUSION AND IMPLICATIONS FOR TRANSLATION
This self-experimentation describes the author’s experiment, which has effectively prevented RTIs for him since 1979, including during the peak period of the COVID-19 pandemic. Despite the potential risks during the pandemic, the author intentionally exposed himself to the virus to test his experiment at the very mature age of 73. Further research, such as robust RCTs/cohort RCTs/cluster randomized trials are necessary to confirm or refute the author’s results. If proven effective, The INVals Method could serve as a strong vaccine ally and have broader clinical implications.
Key Messages
-
The INVals Method using Bernoulli’s principle creates Venturi effect which suctions out the pathogens-laden secretions from nasolacrimal ducts, sinuses, nasal cavities, Eustachian tubes, and upper respiratory tract, and these when swallowed subconsciously are successfully inactivated by the hostile environment of stomach and gastrointestinal tract.
-
The mucociliary clearance is always in the direction of the inlet of the esophagus, downwards from the upper respiratory tract and upwards from the lower respiratory tract. Thus, The INVals Method by suctioning out enhances these movements and helps the natural process of mucociliary clearance.
-
o
Nose blowing markedly increases intranasal pressure, thus propelling pathogens into nasolacrimal ducts, sinuses, and Eustachian tubes causing inflammation, infections, and biofilms formations in these areas.
-
o
The INVals Method can prove to be a vaccine ally, especially in middle- and low-income countries, where there is usually a significant lag period in acquisition and administration of vaccines.
-
o
As The INVals Method involves short periodic exercises throughout the day, it prevents “Exercise Resistance” where fat metabolism is more influenced by the inhibitory effects of sedentary lifestyle.
-
o
Unbiased, rigorous RCTs are warranted before The INVals Method results can be generalized.
-
Acknowledgments
None
COMPLIANCE WITH ETHICAL STANDARDS
Conflicts of Interest
The author declares no competing interests.
Financial Disclosure
There is no financial disclosure to declare.
Funding/Support
There was no outside funding/support for this study.
Ethics Approval
Not applicable.
Declaration of Patient Consent
Not applicable.
Use of Artificial Intelligence (AI)-Assisted Technology for Manuscript Preparation
The author confirms that there was no use of AI-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Disclaimer
The views expressed are the author’s and not necessarily those of any institutions.
REFERENCES
- Accute respiratory infections are world’s third leading cause of death. BMJ. 2010;341:6360.
- [Google Scholar]
- The global burden of lower respiratory infections: Making progress, but we need to do better. Lancet Infect Dis. 2018;18:1162-63.
- [CrossRef] [PubMed] [Google Scholar]
- Infectious disease hospitalizations in the United States. Clin Infect Dis. 2009;49:1025-39.
- [CrossRef] [PubMed] [Google Scholar]
- Lessons from the past: Methodological issues arising from comparison of the disease burden of the influenza A (H1N1) pandemic 2009–10 and seasonal influenza 2010–2019 in the United States. J Infect Dis Epidemiol. 2021;7:218.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Global burden of upper respiratory infections in 204 countries and territories, from 1990 to 2109. EClinical Medicine. ;37:100986.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Systematic review of the efficacy, effectiveness and safety of cell-based seasonal influenza vaccines for the prevention of laboratory-confirmed influenza in individuals ≥ 18 years of age. Rev Med Virol. 2023;33(3):e2332.
- [CrossRef] [PubMed] [Google Scholar]
- Respiratory viral infections in the elderly. Ther Adv Respir Dis. 2021;15:1753466621995050.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- WHO. Tracking SARS-CoV-2 variants. 2023 [Accessed January 19, 2023]. Available from: https://www.who.int/activities/tracking-SARS-CoV-2-variants.
- False-positive results in rapid antigen tests for SARS-CoV-2. JAMA. 2022;327:485-6.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Clinical consensus statement: Diagnosis and management of nasal valve compromise. Otolaryngol Head Neck Surg. 2010;143:48-59.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Bernoulli’s Equation and Venturi Effect. In: Essential Equations for Anaesthesia. Cambridge, UK: Cambridge University Press; 2014. p. :26-28.
- [Google Scholar]
- Airway mucus function and dysfunction. N Engl J Med. 2010;363:2233-47.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Total virus and bacteria concentrations in indoor and outdoor air. Environ Sci Technol Lett. 2015;2:84-8.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Local mucociliary defence mechanisms. Paediatr Respir Rev. 2000;1(1):27-34.
- [CrossRef] [PubMed] [Google Scholar]
- Physiology and pathophysiology of human airway mucus. Physiol Rev. 2022;102(4):1757-836.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- How nasal function influences the eyes, ears, sinuses, and lungs. Proc Am Thorac Soc. 2011;8(1):53-61.
- [CrossRef] [PubMed] [Google Scholar]
- Antimicrobial peptides (AMPs): Ancient compounds that represent novel weapons in the fight against bacteria. Biochem Pharmacol. 2017;133:117-38.
- [CrossRef] [PubMed] [Google Scholar]
- The respiratory microbiome and respiratory infections. J Infect. 2017;74(Suppl 1):S84-8.
- [CrossRef] [PubMed] [Google Scholar]
- Commonality despite exceptional diversity in the baseline human antibody repertoire. Nature. 2019;566(7744):393-7.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Virus cell-to-cell transmission. J Virol. 2010;84(17):8360-8.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Nose blowing propels nasal fluid into the paranasal sinuses. Clin Infect Dis. 2000;30(2):387-91.
- [CrossRef] [PubMed] [Google Scholar]
- Biofilms and inflammation in patients with chronic rhinosinusitis. Med Pharm Rep. 2020;93(4):374-83.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Mucosal immune system of the gastrointestinal tract: Maintaining balance between the good and the bad. Scand J Gastroenterol. 2017;52(11):1185-93.
- [CrossRef] [PubMed] [Google Scholar]
- Gastrointestinal stress as innate defence against microbial attack. J Appl Microbiol. 2021;130(4):1035-61.
- [CrossRef] [PubMed] [Google Scholar]
- Gastric juice: A barrier against infectious diseases. Basic Clin Pharmacol Toxicol. 2005;96(2):94-102.
- [CrossRef] [PubMed] [Google Scholar]
- The mucus and mucins of the goblet cells and enterocytes provide the first defense line of the gastrointestinal tract and interact with the immune system. Immunol Rev. 2014;260(1):8-20.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Intestinal barrier function and metabolic liver diseases. Liver Res. 2020;4:81-7.
- [CrossRef] [Google Scholar]
- The mechanism behind influenza virus cytokine storm. Viruses. 2021;13(7):1362.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Preventing COVID-19, saving lives in lower-income countries. JAMA. 2022;328(7):611.
- [CrossRef] [PubMed] [Google Scholar]
- Should I Breathe Through My Mouth or Through My Nose? 2020 [Accessed February 21, 2023]. Available from: https://health.clevelandclinic.org/breathe-mouth-nose/.
- Human adult deglutition during sleep. Ann Otol Rhinol Laryngol. 2006;155(5):334-9.
- [CrossRef] [PubMed] [Google Scholar]
- Daily step count and postprandial fat metabolism. Medicine and science in sports and exercise. Med Sci Sports Exerc. 2021;53(2):333-40.
- [CrossRef] [PubMed] [Google Scholar]
- Mobile intervention to promote correct hand hygiene at key times to prevent COVID-19 in the swiss adult general population: Study protocol of a multiphase optimisation strategy. BMJ Open. 2022;12(3):e055971.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Facemask and hand hygiene to prevent influenza transmission in households: A cluster randomized trial. Ann Intern Med. 2009;151(7):437-46.
- [CrossRef] [PubMed] [Google Scholar]
- The role of facemasks and hand hygiene in the prevention of influenza transmission in households: Results from a cluster randomized trial; Berlin, Germany, 2009–2011. BMC Infect Dis. 2012;12:26.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- One mutation away, the potential zoonotic threat – neocov, planetary health impacts and the call for sustainability. J Public Health Res. 2022;10(1 Suppl) jphr.2021;2941
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- NeoCoV. A foresight of the next possible pandemic. Int J Surg. 2022;99:106255.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- A global effort to define the human genetics of protective immunity to SARS-CoV-2 infection. Cell. 2020;181(6):1194-9.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Who goes first? The story of self-experimentation in medicine. Rob cowley and carol tarlow (ed). New York: Random House; 1987.




{kind=link}
{kind=link}