

Translate this page into:
Determinants of Under-Five Mortality in Ghana: Evidence from the Ghana Demographic and Health Survey
✉Corresponding author email: albertnyaaba13@yahoo.com
-
Received: ,
Accepted: ,
This article was originally published by Global Health and Education Projects, Inc. and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background and Objectives:
This study aims to investigate the strength of the association between socioeconomic, maternal and environmental determinants and under-five mortality in Ghana.
Methods:
We utilized data from the 2014 Ghana Demographic and Health Survey, a population-based cross-sectional study, which included 4151 children born alive to women aged 15-49 years. The primary outcome variable was under-five mortality. Descriptive statistics and multivariate logistic regression were applied to assess the relationship and relative association of the independent variables with the outcome variable.
Results:
Children of women with secondary education and above and women within the middle wealth status were 0.593 and 0.886 less likely to experience under five deaths compared to women with no education and women of low wealth status (OR=0.593; 95% CI 1.690 to 2.063; p< 0.01) (OR =0.886; 95% CI 1.48 to 1.63; p<0.01). Women who had their first child between the ages of 20-29 were 0.764 less likely to have children die before age 5 compared to those women who had their first child between the ages of 15-19. (OR= 0.764; 95% CI 0.994 to 1.191; p<0.0l). Children born in households with pit toilets were more likely (OR= 1.51; 95% CI 1.20 to 2.30; p<0.01) to die before age five compared to children born in households with flushed toilet. Women who used borehole/well-water were more likely (OR= 1.686; 95% CI 2.94 to 3.01; p< 0.05) to experience under-five deaths compared to women who used piped water.
Conclusion and Implications for Translation:
This study identified the determinants that significantly predicted under-five deaths and the magnitude of the influence on under-five deaths in Ghana. It accentuates the need for increased maternal education, delayed childbearing age, provision of improved drinking water and toilet facilities to reduce under-five deaths in Ghana.
Keywords
Socioeconomic
Maternal Health
Child Health
Environmental Factors
Under-five Mortality
Ghana
Demographic and Health Survey
DHS

1. Background
Under-five mortality is a major indicator of child health, healthcare, and the overall development of every nation because it depicts the social, economic, and environmental conditions in which children are born.1 Under-five mortality is defined as the risk of a child dying before completing five years of age.2 The 21st century has witnessed the most dramatic decline in under-five mortality in almost all countries of the world, regardless of initial levels, socioeconomic circumstances and development strategies.3 Globally, under-five mortality rates per 1000 live-births has fallen from 90.6 deaths in 1990 to 42.5 in 2015.4
Despite this decline, more than 10.8 million under-five deaths have occurred in 2014 mostly from preventable causes.11 The leading causes of death among children under-five have been attributed to preterm birth complications, acute respiratory infections, intrapartum-related complications, congenital anomalies, diarrhea and malaria.5 Between 2016 and 2030, 94.4 million children are projected to die before age five years if the 2015 mortality rate remains constant in each country whereas 68.8 million would die if each country continues to reduce its mortality rate at the pace estimated from 2000 to 2015.4 The overwhelming majority of these deaths occurred in the poorest regions and countries of the world, and in the most underprivileged areas within countries.6 Under-five deaths is still a major public health problem in developing countries, especially in Sub-Saharan Africa where the rates have been persistently higher compared to other regions from 1990 to 2016.7 However, all countries have been benchmarked to reduce under-five mortality to at least 25 deaths per 1000 live-births by 2030 according to the Sustainable Development Goal (SDG) 3 target 2.8
According to estimates from the Global Burden of Disease (GBD), 2017 SDG Collaborators, many countries are on track for achieving the target of at least 25 deaths per 1000 livebirths by 2030. However, about 31 countries would need to achieve annual rates of decline from 2015 to 2030 that are about two to ten times higher than what was recorded for 1990-2015 in order to achieve this goal.9 In spite of the significant decline in global under-five mortality, the rates remain high in Sub-Saharan Africa where many countries, such as Ghana, failed to meet the Millennium Development Goals (MDGs) Goal 4 which aimed at achieving a two-thirds reduction in the under-five mortality rate by 2015. For example, in 2015, the under-five mortality rate in Sub-Saharan Africa was 79 deaths per 1000 live births compared to the global rate of 41 deaths per 1000 live births in the referenced year.4
Within sub-Saharan Africa, Ghana in particular, experienced a slow, but nevertheless, steady decline in its under-five mortality rate over the past 40 years with an accelerated reduction since the year 2000. Despite the decline, under-five mortality rate in Ghana is still high with a rate of 60 deaths per 1000 live births as of 2014. This fell short of the target set in the Ghana Under-five Child Health Policy 2007—2015 which targeted a reduction in under-five mortality to 40 deaths per 1000 live births by 20I5.10 Though Ghana has made some significant progress in under-five mortality, the improvement is widely due to governments' commitment to improved services, poverty reduction and various new targets of public health initiatives that have improved access to water and sanitation, maternal health and child health.11 Other programs included the community health planning services program, (CHPS) established in 2006 which sought to provide access, quality and equitable health care services and the National Health Insurance Scheme (NHIS) established in 2003 with the goal of providing financial access to healthcare services.12
Despite all these interventions, under-five mortality remains high. A recent study of 46 African countries showed that Ghana is among the eight countries not making enough efforts towards reducing under-five mortality.13 Further investigation into the factors influencing the under-five mortality is therefore warranted. In order to achieve the SDGs 3.2, understanding of determinants of under- five mortality and the implementation of appropriate intervention is expected from countries with high under-five mortality. In Ghana, a few studies have examined the factors influencing under-five mortality. Tette et al.14 conducted a health facility-based case control studies in Accra, Ghana to examine the risk factors associated with under-five mortality in the country. This study was not representative of under- five deaths in the general Ghanaian population. Quansah et al.15 conducted a systematic review on social factors influencing under-five mortality; Kanmiki et al.16 investigated the socioeconomic and demographic determinants of under-five mortality, whilst Aheto7 studied predictive model and determinants of under-five mortality. Thus, there is limited information published on socioeconomic, maternal and environmental factors influencing under-five mortality in Ghana.
To guide our study, we adopted a conceptual framework by Mosley and Chen17 on socioeconomic and proximate determinants of mortality. According to this framework, the socioeconomic factors such as work status, wealth quintile, and education indirectly affect the under-five mortality through the operations of the proximate determinants of maternal, environmental, nutritional, injury and behavioral factors. The limitation of this framework, however, was that not all the variables are applicable in all settings hence the need for the adaptation (Figure 1).
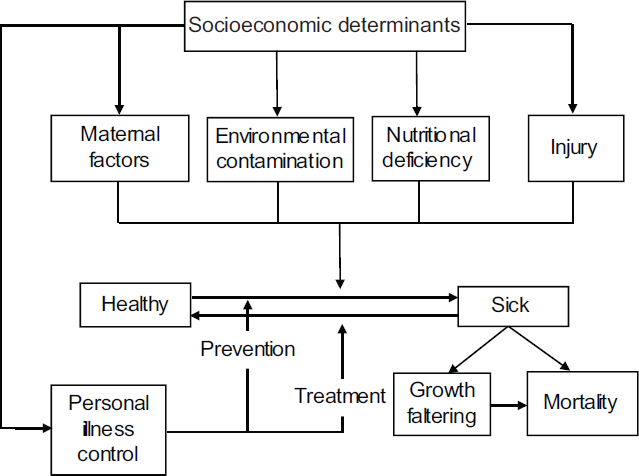
- Proximate determinants of child survival
- Source: Adapted from Mosley and Chen, 1984
To assess child survival programs, the socioeconomic and proximate determinants of under-five mortality should be measured in a population-based research. Based on the on-going debate on the influence of particular socioeconomic, maternal and environmental characteristics of mothers on under-five mortality in Ghana, this paper sought to investigate further the socioeconomic, maternal and environmental factors that influence under five mortality and the magnitude of their influence in Ghana using a nationally representative dataset.
2. Method
2.1. Study Design and Sampling
This study used data from the 2014 Ghana Demographic and Health Survey (GDHS) conducted in Ghana every five years. The GDHS collects nationally representative data on women of child-bearing age (15-49) years and their children.10
The data were obtained from the DHS MEASURE Program (Measure DHS) which is readily available online and contains information which covers a range of population, health, fertility and nutrition indicators such as childhood mortality, maternal and child health, use of family planning methods, nutritional status of women and children as well as household socioeconomic variables.10 The GDHS focuses on child and maternal health and is designed to provide adequate data to monitor the population and health situation in Ghana. It employed a two-stage sample design to select respondents for the study. The 2014 round of survey interviewed 9396 women aged within 15-49 years from 12,831 households covering 427 clusters comprising 216 and 211 urban and rural areas respectively. It had a response rate of 97 percent.11 Detailed survey methods are published and available online.11 Data on children less than five years who were born five years preceding the survey were 4151 on which the analyses were based. Complete birth histories were collected including month and year of each child's birth and death. These data were used to identify the number of children born in the last five years and age at death.
2.2. Measures
The dependent variable for the study was under-five mortality, coded “1” if a child died before the fifth birthday and “0” if otherwise. The responses were dichotomously coded as Yes or No. The determinants examined in the study were selected based on the literature and included age of mother at first birth, grouped as 15-19, 20-29 and 30-39 years; mother's level of education, categorized as no education, primary education and secondary education and above; wealth status grouped as low, middle and high; birth order of child grouped as 1,2-3, and 4+; birth interval as <24 month and > 24 months; place of delivery put into home, public facility, private facility and others; type of toilet recoded as flushed, pit toilet and others; source of drinking water was also recoded as piped water, borehole and others.
2.3. Statistical Analysis
Descriptive statistics as well as a chi-square test were used to examine the distribution of under- five mortality by the selected characteristics, whilst binary logistic regression was employed to identify significant covariates associated with the probability of dying before age 5 years. A sequential modelling technique was adopted to examine the extent to which the selected socioeconomic, maternal and environmental factors contribute to explain the variation in the probability of a child dying before age 5. Model 1, accounting for only the socioeconomic factors (educational level, work status and wealth) was then fitted. Model 2 included the maternal factors (age at first birth, birth order, birth interval and place of delivery), whilst the environmental factors (toilet facility and source of drinking water) were added in Model 3. The models conducted were expressed as odds ratios at the corresponding 95% confidence intervals. In computing the odds ratio for each category of the independent variables, multicollinearity was checked with variance-inflation factor (VIF) and a mean value of 1.26 found indicating the absence of multi collinearity (VIF above 10 indicates the presence of multicollinearity).18 The Ethics Review Committee, Ghana Health Service, Accra, Ghana and the Ethics Committee of ICF Macro in Calverton, USA gave the ethical approval to conduct GDHS which was used in this study.
3. Results
3.1. Characteristics of the Population
General characteristics of the population are shown in Table 1 below. About 9396 women aged 15-49 years were interviewed from 12 831 households. About 47% of the women had secondary education and above with almost 80% categorized as currently working. More than half (52%) of the women were found in low wealth quintile. Approximately three percent of the live births died before age five.
| Variable | Alive (%) | Dead (%) | Total |
|---|---|---|---|
| Children under-five | 4031 | 120 | 4151 |
| Highest education | X2=2. 0432 d=2 | Pr=0.036 | |
| No education | 96.8 | 3.2 | 1355 (100) |
| Primary education | 97.8 | 2.2 | 857 (100) |
| Secondary education above | 97 | 3 | 1960 (100) |
| Work status | X2=0. 0532 d=1 | Pr=0.818 | |
| Currently working | 96.9 | 3.1 | 854 (100) |
| Not working | 96.9 | 3.1 | 3123 (100) |
| Wealth status | X2=0.8928 d=2 | Pr=0.048 | |
| Low | 97.1 | 2.9 | 2137 (100) |
| Middle | 96.5 | 3.5 | 797 (100) |
| High | 97.3 | 2.7 | 1217 (100) |
| Place of delivery | X2=1.5775 d=3 | Pr=0.665 | |
| Home | 97.4 | 2.6 | 1124 (100) |
| Public facility | 96.9 | 3.1 | 2738 (100) |
| Private facility | 97.4 | 2.6 | 272 (100) |
| Other | 93.3 | 6.7 | 16 (100) |
| Age at first birth | X2=1.5903 d= 2 | Pr=0. 462 | |
| 15-19 | 97.4 | 2.6 | 1838 (100) |
| 20-29 | 96.9 | 3.1 | 2167 (100) |
| 30-39 | 95.7 | 4.3 | 144 (100) |
| Birth order | X2=3. 4591 d=2 | Pr=0.027 | |
| 1 | 96.4 | 3.6 | 929 (100) |
| 2-3 | 98.3 | 1.7 | 1526 (100) |
| 4+ | 97 | 3 | 1694 (100) |
| Birth interval | X2=0.3620 d=1 | Pr=0.470 | |
| <24 Months | 96.7 | 3.3 | 411 (100) |
| >24Months | 97.3 | 2.7 | 2796 (100) |
| Type of toilet | X2=5. 2702 d=4 | Pr=0.026 | |
| Flush toilet | 98 | 2 | 560 (100) |
| Pit toilet | 96.8 | 3.2 | 2218 (100) |
| Other | 97.1 | 2.9 | 1371 (100) |
| Source of drinking water | X2=4.1095 d=2 | Pr=0.350 | |
| Piped water | 96.5 | 3.5 | 1140 (100) |
| borehole/well-water | 97 | 3 | 1396 (100) |
| Other | 97.5 | 2.5 | 1613 (100) |
Source: Data computed from the GDHS, 2014
3.2. Relationship between the Determinants and Under-five Deaths
Table 1 shows the results of chi-square analysis that examined the relationship between the determinants and the outcome. For the socioeconomic determinants, maternal education had significant relationship with under-five deaths (X2=2.0432; p=0.036). The highest (3.2%) proportion of under- five deaths, were observed among mothers with no education. Wealth status was found significant with under-five deaths (X2=0.8928; p=0.048) with children born to mothers in middle wealth quintile households recording 3.5 % under-five deaths. Maternal determinants indicated that birth order was significantly associated with under-five mortality (X2=3.4559l; p=0.027). With respect to environmental determinants, type of toilet facility was significantly associated with under-five deaths (X2=5.2702; p=0.026). However, most (3.2%) under- five deaths were accounted for by households using pit toilet facility (Table 1).
3.3. Socioeconomic Status, Maternal and Environmental Determinants and Under-five Deaths
Table 2 shows results of multivariate logistic regression (sequential model) that examined association between socioeconomic, maternal and environmental factors and under-five death. Conducted to identify the determinants of under- five mortality, the models indicated pseudo R2 values for the three models considered in the analyses as Model l (socioeconomic factors) - 0.103; Model II (maternal factors) - 0.170; and Model III (socioeconomic factors, maternal factors and environmental factors) - 0.270. The fit of a model was also expressed by the coefficient of regression (pseudo R2). It showed that Model III best explained the contribution of the covariates to under-five mortality. The results indicated that in Model I, education and wealth status were significantly associated with under five mortality. In Model II, wealth, age at first birth, place of delivery were significant whilst in Model III, education, wealth status, age at first birth, birth order, place of delivery, type of toilet facility and source of drinking water were all significant at different confidence intervals. This implies that children born to women with secondary education and above were 59% less likely to experience under-five mortality compared to children born to women with no education (OR=0.593; 95% CI 1.690 to 2.063; p<0.05). Children born to women who gave birth to their first child at age 20-29 years were 76 % less likely to die before age five compared to those 15-19 years (OR= 0.764; 95% CI 0.940 to 1.191; p< 0.01). On wealth status, children born to household within the middle wealth status were almost 89% likely of dying before age five compared to children born to low wealth status households (OR=0.886; 95% CI 0.481 to 1.632; p<0.01). Regarding birth order, children born to order 4+ were 66% less likely to experience under five deaths (OR=0.662; 95% CI 1.710 to 2.24; p<0.01) compared to birth order 1. The likelihood of under five deaths among children born in the public health facility was 67% less (OR=0.670; 95% CI 1.395 to 2.136; p<0.001) compared to those born at home. Conversely, children born to households using pit toilet were 51% (OR=0.51; 95% CI 1.201 to 2.303; p<0.01) more likely to die before age five compared to children in households using flushed toilet. About 69% of children born to households with borehole as their main source of drinking water were more likely to die compared to children of household using piped water (OR=1.686; 95% CI 2.942to 3.015; p<0.05) (see Table 2).
| Variables | Model I Odds ratio | Model II Odds ratio | Model III Odds ratio |
|---|---|---|---|
| [Confidence Interval] | [Confidence Interval] | [Confidence Interval] | |
| Socioeconomic determinants | |||
| Education | |||
| No education | Ref. | Ref. | Ref. |
| Primary education | 1.511 | 1.805 | 1.777 |
| [0.860,2.655] | [0.929,3.506] | [0.911,3.466] | |
| Secondary education above+ | 0.703* | 0.246 | 0.593** |
| [0.678,1.699] | [0.725,2.144] | [1.690,2.063] | |
| Work status | |||
| Currently working | Ref. | Ref. | Ref. |
| Not working | 1.046 | 1.225 | 1.175 |
| [0.671,1.631] | [0.701,2.143] | [0.671,2.060] | |
| Wealth | |||
| Low | Ref. | Ref. | Ref. |
| Middle | 0.812* | 0.760* | 0.886** |
| [0.499,1.322] | [0.430,1.343] | [0.481,1.632] | |
| High | 1.040 | 1.219 | 1.182 |
| [0.636,1.700] | [0.644,2.308] | [0.578,2.419] | |
| Maternal determinants | |||
| Age at first birth | |||
| 15-19 | Ref. | Ref. | |
| 20-29 | 0.778* | 0.764** | |
| [0.499,1.214] | [0.490,1.191] | ||
| 30-39 | 0.858 | 0.770 | |
| [0.197,3.739] | [0.176,3.381] | ||
| Birth order | Ref. | Ref. | |
| 1 | 1.569 [0.881,2.79] | 1.343 [0.848,2.125] | |
| 2-3 | 0.737 | 0.662** | |
| 4+ | [0.466,1.166] | [1.710,2.24] | |
| Birth interval | |||
| Ref. | Ref. | ||
| <24 Months | [0.438,1.468] | [0.688,2.315] | |
| >24 Months | 0.802 | 1.262 | |
| Place of delivery | |||
| Home | Ref. | Ref. | |
| Public facility | 0.651** | 0.670*** | |
| [0.384,1.103] | [1.395,2.136] | ||
| Private facility | 0.239 | 0.145 | |
| [0.351,4.370] | [0.323,4.053] | ||
| Other | 0.295 | 0.320 | |
| [0.0363,2.399] | [0.0390,2.617] | ||
| Environmental determinants | |||
| Flush toilet | Ref. | ||
| Pit toilet | 1.512** | ||
| [1.201,2.303] | |||
| Other | 0.505 | ||
| [0.177,1.440] | |||
| Source of drinking water | |||
| Piped water | Ref. | ||
| Borehole/well-water | 1.686* | ||
| [2.942,3.015] | |||
| Other | 1.494 | ||
| [0.874,2.553] | |||
| N | 4151 | 4151 | 4151 |
| Pseudo r2 | 0.103 | 0.170 | 0.270 |
Exponentiated coefficients; Cl-Confidence Interval; 95% Confidence Intervals in brackets Ref.=Reference category
Source: Data computed from the GDHS 2014
4. Discussion
This study examined the influence of socioeconomic, maternal and environmental characteristics on mothers of children who experienced under-five mortality in Ghana. The bivariate analysis in Table 1 showed that education, birth order and type of toilet facility used had significant relationship with under-five mortality. Results of multivariate analysis indicated that multiplicity of factors are involved in under-five mortality. Education was significantly associated with under-five mortality. Children of mothers who had secondary education and above were less likely to experience under-five mortality compared to mothers with no education. This finding is consistent with those by Worku19 that under-five mortality rates were higher among less-educated mothers compared with mothers who have higher levels of education. This could be attributed to the fact that mothers who are educated are more likely to take their children to a health center for preventive and curative care to avoid the delays as posited in the three-delay model.20 In view of this, the government's free senior high school policy introduced in the 2017/2018 academic year should be well-managed due to the great benefit to mothers age 15-19.21
Regarding wealth status, the finding show that children born to mothers from households within the middle wealth status were of less likelihood of under-five mortality compared to those of low wealth status. These findings affirmed what Doctor et al.,22 found that children in the low wealth status households were more likely to die before reaching their fifth birthday compared to those in the middle and high wealth households. This is because rich households are able to afford food that is necessary for under-five growth which improves their immunity and help in reducing infections which are a major threat to the child's survival. They could also access quality healthcare which is important for child survival but not the case for households in low wealth status. The effects of age at first birth on child health have been a subject of extensive discourse in literature. Findings of this study revealed that children born to mothers aged 30-39 years were less likely to experience under-five mortality compared to mothers aged 15-19 years. This confirms studies by Kayode et al.,23 that children of mothers who started childbearing at an early age (15-19) were more prone to experience under-five mortality compared to those that commenced childbearing at an older age (30-39). This may be explained by the fact that mothers of this age group are mature, have access to health care and tend to utilize health information. Therefore, the Adolescent Health Service Policy and Strategy 2016-2020 should be refreshed and properly implemented emphasizing contraception and abstinence so as to delay child bearing.24
Contrary to previous studies by Hossain et al.,25 which found that birth order 4+ have higher risk of mortality compared to lower birth orders, this study found that children born to order 4+ were less likely to die before age five compared to order 1, perhaps mothers of these children are mature (20-39), experienced and make some advance preparations before delivery.
In connection with place of delivery, children who were born in public facilities were less likely to die before reaching their fifth birth day compared to those born at home. This finding supports studies by Sahu et al.26 that delivery at a health facility reduces the risk of under-five mortality. As a result, the free maternal health policy was implemented under the National Health Insurance Scheme in Ghana in 2008.27 The policy guarantees all pregnant women to have free registration with the National Health Insurance Scheme (NHIS) after which they would be entitled to free services throughout pregnancy, childbirth and three months postpartum. The reason being that, health facilities have professional service providers who take good care of the health needs of both the mother and the newborn. Studies have shown that women's decisions about the choice of place of birth either at the facility or home are influenced by several factors, ranging from demographic, socioeconomic circumstances, cultural to health system factors28 in an attempt address this, the Community-based Planning and Health Services was introduced in 1994 with the aim of bringing health care close to communities.24 Determining the effects based on the source of drinking water, children born to mothers from households using borehole/well-water as their major source of drinking water were 67% more likely to experience under-five mortality compared to those children of households using piped water. This supports findings by Kayode et al.23 that availability of piped water in a dwelling has a positive influence on child survival. This may be due in part to the undeveloped immune system of children meriting them more susceptible to water-borne infections.
The risk of under-five mortality to children from households with no toilet facility were more likely compared to households with flushed toilet. This finding supports previous studies that children born to households with toilet facility have reduced relative risks of under-five mortality compared to their counterparts born to households with no toilet facility.29 It is probable that the lack of improved toilet facilities creates unhygienic human waste disposal thereby leading to infections such as cholera or repeated diarrhea which subsequently gives rise to malnutrition, poor health and eventual under-five death. Though, the study did not find work status and birth interval significant, the odds ratio showed that non-working women were more likely to have their children die before age five and children born to women of birth interval >24 months were less likely to die before celebrating their fifth birthday.
4.1. Strengths and Limitations of the Study
This study used nationally representative data from the 2014 Ghana Demographic and Health Survey with robust sampling technique, standardized data collection procedures, high quality interviewer training and high response rate. The biases in the data set were fairly random, the aggregate estimates of indicators were fairly adequate. The study assessed the determinants of under-five mortality on the basis of variables captured in the GDHS data set. Limitations of the survey data includes misclassification since most of the health information were based on women reports. The survey data was also subject to age misreporting since respondents could heap or report their ages on the basis of digit preference.
5. Conclusions and Implications for Translation
This study adds to the understanding of drivers of under-five mortality in Ghana. The evidence of greater risk of under-five mortality associated with early child birth, low wealth status, no education, use of pit toilet facility, lower birth order and use of unimproved source of drinking water underscore the need for toilet facility interventions to address these factors in Ghana. It is recommended that government scale up the WASH toilet project to all part of the country. There is also an urgent need for portable water especially in the rural communities in Ghana. On the basis of the findings, it is recommended that policy makers should not just encourage education of females (15-19 years) but rather emphasize on higher female education beyond primary school level to delay early childbearing. Also, there is the need to promote health facility delivery since it reduces the risk of under-five mortality as a result of the availability of professional service providers who take good care of the health needs of both the mother and the newborn. Findings of this study will inform and strengthen appropriate national policies and intervention strategies aimed at reducing under- five mortality in Ghana in our efforts to achieve the SDG 3.2. It will be worthwhile to research further using qualitative studies to explore the perception of women on why these factors influence under-five mortality in Ghana.
Ethical Considerations
Conflicts of interest:
None.
Ethics Approval:
Ethics Review Committee, Ghana Health Service, Accra, Ghana and the Ethics Committee of ICF Macro in Calverton, USA gave the ethical approval to conduct GDHS.
Financial Disclosure:
Nothing to declare.
Disclaimer:
None
Acknowledgment:
The authors are thankful to Measure DHS for granting them permission to use the GDHS data set.
Funding/Support:
The publication of this article was partially supported by the Global Health and Education Projects, Inc. (GHEP) through the Emerging Scholars Grant Program (ESGP). The information, contents, and conclusions are those of the authors’ and should not be construed as the official position or policy of, nor should any endorsements be inferred by ESGP or GHEP.
References
- Basic health care provision and under-5 mortality: a cross-national study of developing countries. World Dev.. 2006;34(3):405-425.
- [CrossRef] [Google Scholar]
- The Global Health Observatory. WHO; https://www.who.int/data/gho (accessed )
- The decline in child mortality: a reappraisal. Bull World Health Organ. 2000;78(l0):ll75-9l.
- [Google Scholar]
- United Nations Inter-agency Group for Child Mortality Estimation (UN IGME) In: Levels and Trends in Child Mortality. United Nations Children's Fund; 2015.
- [Google Scholar]
- Global, regional, and national causes of under-5 mortality in 2000-15: an updated systematic analysis with implications for the sustainable development goals. Lancet.. 20l6;388(l0063):3027-35.
- [CrossRef] [PubMed] [Google Scholar]
- United Nations Dept. of Economic and Social Affairs: Population Group. 2015. Levels and Trends in Child Mortality: Report 2015. UN; https://www.un.org/en/development/desa/population/publications/mortality/child-mortality-report-20l5.asp (accessed )
- [Google Scholar]
- Predictive model and determinants of under-five child mortality: evidence from the 2014 Ghana demographic and health survey. BMC Public Health.. 20l9;l9(1):64.
- [CrossRef] [PubMed] [Google Scholar]
- Measuring progress from 1990 to 2017 and projecting attainment to 2030 of the health-related Sustainable Development Goals for l95 countries and territories: a systematic analysis for the Global Burden of Disease Study 20l7 Lancet. . 2018;392(10159):2091-2138. doi:10.1016/ S0140-6736(18)32281-5
- [Google Scholar]
- GBD 20l7 Mortality Collaborators. Global, regional, and national age-sex-specific mortality and life expectancy, 1950-2017: a systematic analysis for the Global Burden of Disease Study 20l7. Lancet. 2018;392(10159):1684-1735. doi: 10.1016/S0140- 6736(18)31891-9
- [Google Scholar]
- Ghana Statistical Service, Ghana Health Service, ICF International. 2015. Ghana Demographic and Health Survey 2014. Rockville, Maryland, USA: GSS, GHS, ICF International; https://dhsprogram.com/pubs/pdf/FR307/FR307.pdf (accessed )
- [Google Scholar]
- Country Health Profile 2012. 2012. WHO; www.who.int/whosis/countryselect.cfm (accessed )
- [Google Scholar]
- The effect of Ghana's national health insurance scheme on health care utilization. Ghana Med J. 2012;46(2):76-84.
- [Google Scholar]
- Factors associated with declining under-five mortality rates from 2000 to 2013: an ecological analysis of 46 African countries. BMJ Open. 2016;6(1):e007675. doi: 10.1136/bmjopen-2015-007675
- [CrossRef] [PubMed] [Google Scholar]
- Under- five mortality pattern and associated risk factors: a case-control study at the Princess Marie Louise Children's Hospital in Accra, Ghana. BMC Pediatr. 2016;16(1):148. doi: 10.1186/s12887-016-0682-y
- [CrossRef] [PubMed] [Google Scholar]
- Social factors influencing child health in Ghana. PLoS One. 2016;11(1):e0145401. doi: 10.1371/ journal.pone.0145401
- [CrossRef] [PubMed] [Google Scholar]
- Socioeconomic and demographic determinants of under-five mortality in rural northern Ghana. BMC Int Health Hum Rights. 2014;14:24. doi: 10.1186/1472- 698X-14-24
- [CrossRef] [PubMed] [Google Scholar]
- An analytical framework for the study of child survival in developing countries. Popul Dev Rev (10):25-45.
- [CrossRef] [Google Scholar]
- Factors that affect under-five mortality among South African children: analysis of the South African Demographic and Health Survey Data Set. In: Proceedings of the World Congress on Engineering and Computer Science 2009. San Francisco CA; 2009. p. :1-3.
- [Google Scholar]
- Too far to walk: maternal mortality in context. Soc Sci Med. 1994;38(8):1091-1110. doi: 10.1016/0277-9536(94)90226-7
- [CrossRef] [PubMed] [Google Scholar]
- Policy brief:an appraisal of the free senior high school policy in Ghana. Northern Network for Policy Development. http://www.nnedghana.org/2018/04/19/policy-brief-an-appraisal-of-the-free-senior-high-school-policy-in-ghana/ (accessed )
- [Google Scholar]
- Does living in a female-headed household lower child mortality? The case of rural Nigeria. 2011. Rural Remote Health. 11:1635. http://www.rrh.org.au/articles/subviewnew.asp?ArticleID=1635 (accessed )
- [CrossRef] [PubMed] [Google Scholar]
- Risk factors and a predictive model for under-five mortality in Nigeria: evidence from Nigeria demographic and health survey. BMC Pregnancy Childbirth. 2012;12(1):16-20. doi:10.1186/1471-2393-12-10
- [CrossRef] [PubMed] [Google Scholar]
- Ghana Health Service. Community-Based Health Planning and Services: The Operational Policy. Policy Document No. 20. Ghana Health Service 2005
- [Google Scholar]
- Effects of demographic and household variables on infant and child under-five mortality: an application of logistic model. Internet J Health.. 2008;8(2):2-13.
- [CrossRef] [Google Scholar]
- Levels, trends & predictors of infant and child mortality among Scheduled Tribes in rural India. Indian J Med Res. 2015;141(5):709-719. doi: 10.4103/0971- 5916.159593
- [Google Scholar]
- National Health Insurance Authority (NHIA) In: Annual Report 2009. Accra, Ghana: National Health Insurance Authority; 2010.
- [Google Scholar]
- Barriers to access of maternity care in kenya: a social perspective. J Obstet Gynaecol Can. 2013;35(2):125-130. doi: 10.1016/S1701-2163(15)31016-1
- [CrossRef] [PubMed] [Google Scholar]
- Health situation in the Americas: basic indicators. Washington DC: WHO; http://iris.paho.org/xmlui/handle/l23456789/34329 (accessed )
- [Google Scholar]



