

Translate this page into:
Levels, Trends, and Causes of Adolescent and Young Adult Maternal Mortality in Nigeria During 1990-2017: Analysis of the 2017 Global Burden of Disease Study Database
✉Corresponding author email: jumainmadu@gmail.com
Abstract
Background:
Despite the global progress made in reducing maternal mortality in the past two decades, the health of adolescents and young adult women (10-24 years) has been neglected based on the wrong assumption that they are healthy, especially in a developing country like Nigeria; this is despite the fact that adolescents and young adults (AYA) constitute over 16% of Nigeria's population. Thus, this study aimed to determine the levels, trends, and causes of maternal mortality among AYA women aged 10-24 years in Nigeria.
Methods:
This was a cross-sectional study that utilized secondary data sets running from 1990 to 2017 from the Global Burden of Disease Study's (GBD) online interactive tool downloaded from the Global Health Data Exchange (GHDx) platform. From the database, we extracted the numbers of maternal deaths (10-49 years), adolescent and young adults' maternal deaths (10-24 years), the proportion of maternal deaths (10-24 years), and both maternal mortality ratio and rate for 15-49 years old and 10-24 years old in the form of Comma separated values (CSV) and converted into XLS file in Microsoft (MS) Excel format for the analysis. Frequencies, proportions, and charts were generated using MS Excel.
Result:
A total of 122,107 maternal deaths occurred among adolescents and young adults (AYA), which is 26% of all deaths occurring among 10-49 years old. Year-to-year changes in the absolute numbers of maternal deaths among AYA showed that it ranged from 3,866 (1990) to 4,451 (2017), showing a slight upward increase over the period; however, both AYA maternal mortality ratio and rate show consistent declines over the period. AYA maternal mortality ratio (MMR) for adolescents aged 15-19 years was 17% higher than for young adults aged 20-24 years. Sepsis was the leading cause of adolescent maternal death (MMR of 168), followed by maternal hypertensive disorder, obstructed labor, maternal hemorrhage, ectopic pregnancy, and abortion. A total of 460,155 maternal deaths occurred in women aged 10-49 years during the study period. Maternal deaths in the age group 10-24 years ranged from 3,866 (29.8%) in 1990 to 4,451 (25.1%) in 2017. The maternal mortality ratio in women aged 10-49 years declined by about 30% for the 1990 – 2017 period.
Conclusion and Implications for Translation:
The study showed that adolescents and young adults are at increased risk of maternal deaths in Nigeria. Therefore, multi-faceted maternal health programs in the country need to target this age group to prevent maternal deaths.
Keywords
Maternal Mortality
Nigeria
Ratio
Rate
Adolescent
Young Adult
GBD
Trend

Introduction
Worldwide, substantial progress has been made in the reduction of maternal mortality since the setting of the Millennium Development Goals (MDGs) in 2000.1 There was a 38% reduction in maternal mortality ratio (MMR) between 2000 and 2017, an average annual rate of reduction of 2.9%.2 A particular age group (adolescents and young adults) appears to have been neglected in measuring progress towards preventing and ending maternal mortality simply because of the assumption that they are healthy.3 Globally, the current population of this vulnerable group (10-24 years old) is estimated at 1.85 billion or 23.7% of the world population, with female adolescents and young adults (AYA) constituting about 49%; 90% of whom live in low- and middle-income countries.4 This population group is considered vulnerable due to the wrong assumption that they are healthy despite the fact that preventable diseases and mortality rates from diseases such as HIV, injury, tuberculosis, maternal conditions, and mental disorders are higher compared to other population groups (25-49 years).5-8 Additionally, risky lifestyle behaviors (e.g., tobacco smoking, alcohol intake, illicit substance abuse) adopted during this period of development lead to the emergence of chronic non-communicable diseases later in life.9,10
Thus, there is a need to focus attention on the health status of this group aside from their population size.3 Firstly, their current health status determines the future health status of the population to a greater extent. Secondly, they are largely responsible for the future pattern and level of social and economic development in sub-national, national and international arenas.5 Thirdly, risk factors and lifestyles adopted during this period will shape the emergence of other risk factors and diseases such as physical inactivity, sexual behaviors, substance abuse, and drug addiction in the future. For example, physical activity such as regular exercise, adopted during this period, has been found to be protective against cardiovascular diseases and diabetes mellitus.6-7 Fourthly, which is a part of the focus of this paper, female adolescents and young adults face various forms of health, socioeconomic and socio-demographic challenges despite international declarations to address them.8,9 For instance, an estimated 2.6 million deaths occurred among AYA in 2004, of which maternal conditions were the leading causes of female deaths at 15%.3 The risk of maternal death among AYA is estimated at 28% higher for women aged 15-19 years compared to those aged 20-24 years.3 Similarly, a systematic review of data from 144 countries reported higher MMR among adolescents aged 15-19 years (260 per 100,000) compared with women aged 20–24 years (190 per 100,000).10 Typically, the maternal mortality rate across the spectrum of childbearing age has been described as a ‘J-shaped’ curve, with higher risks associated with adolescents and young adults, a nadir at 20-29 years, and risk increasing steadily to 49 years.10
In Nigeria, there is a paucity of data on the systematic analysis of maternal deaths among adolescents and young women (AYW). While the studies by Nove et al. and Blanc et al. have included Nigeria, studies primarily focusing on Nigeria to assess the levels, changes over time on causes of adolescent maternal deaths have not been conducted to the best knowledge of the authors.10,11 However, hospital-based studies have been conducted but have the limitations of small data sets, lack of national representativeness and bias inherent with hospital-based studies in the form selection bias of the sample/respondents.12-15 Furthermore, aside from fragmentary hospital-based studies, little is known about the level, pattern, and causes of adolescent maternal mortality either from small-scale population-based research or from a nationally-representative sample survey. Therefore, this study used large data sets from the Global Burden of Disease (GBD) Study led and produced by the Institute of Health Metrics and Evaluation (IHME) at the University of Washington, USA to overcome these gaps and deficiencies. GBD is a global effort that created a platform to compare the quantum of diseases, injuries, and risk factors across age groups, sexes, countries, and time that can be accessed and used by policymakers, health program managers, and researchers within and between countries for comparison. It also allows us to understand and quantify leading causes of death as well as risk factors to our health such as air pollution, sedentary life, tobacco smoking, lack of clean water, and poor nutrition/unhealthy diets. Thus, in the absence of nationally representative data (such as reliable and accurate census data or civil registration data) over a long period of time (say 10-20 years), GBD provides a robust alternative to quantify the level, pattern, and causes of maternal deaths among the adolescents and young adults (AYA) in many countries across the globe including Nigeria from 1990 to 2017.16 For decision-makers, health sector leaders, researchers, and informed citizens, the GBD approach provides an opportunity to compare their countries' health progress to that of other countries, and to understand the leading causes of health loss that could potentially be avoided, like high blood pressure, smoking, and household air pollution. In the same vein, this study aimed to determine the levels, trends, and causes of maternal deaths among adolescents and young women in Nigeria using the GBD Study data points between 1990 and 2017.
Methods
Data and Data Source
We extracted the numbers of maternal deaths (10-49 years), adolescents and young adults' maternal deaths (10-24 years), the proportion of maternal deaths (10-24 years); and maternal mortality ratio and rate for aged 15-49 years and adolescent and young adult maternal mortality rate and ratio (10-24 years) from the database. The Institute of Health Metrics and Evaluation (IHME) at Washington University provides the dataset freely with a user-friendly interface, the GBD Results Tool on the Global Health Data Exchange (GHDx) platform.17 The tool allows users to submit queries and download data files in CSV formats of indicators published on the GBD website. Briefly, the GBD Study generates the most up-to-date account of the causes of deaths and disability using a number of available datasets and statistical models, registration data and sample registration systems, and data from census and surveys. The study is compliant with interactive visualizations for all-cause mortality as well as age- and sex-specific cause mortality for 204 countries and territories, compiling 369 diseases and injuries and 87 risk factors. Additional details on GBD methodologies are published elsewhere.18 Data for Nigeria for years running from 1990 to 2017 were freely downloaded and analyzed.
Health Indicators and Outcomes
We considered the following health indicators from the Global Health Data Exchange (GHDx) platform: maternal mortality ratios (defined as the number of maternal deaths during a given time period per 100,000 live births during the same time period), maternal mortality rates (defined as the number of maternal deaths during a given time period per 100,000 women aged between 15 and 49 years during the same time period) and maternal deaths (defined as the death of a female from any cause related to or aggravated by pregnancy or its management- excluding accidental or incidental causes- during pregnancy and childbirth or within 42 days of termination of pregnancy, irrespective of the duration and site of the pregnancy for a specified time period) for subsets of ages between 10 and 24 years with sub-categorization of 10-14, 15-19, and 20-24 years; female; and maternal disorders as the cause of death (with a code identified as A.6.1).
Statistical Methods
For this study, data from 1990 to 2017 were retrieved. Seven data points were also presented: 1990, 1995, 2000, 2005, 2010, 2015, and 2017. We downloaded the relevant data points from the GHDx platform in CSV formats and subsequently converted them into XLS for analysis. We analyzed the data in MS Excel to generate frequency tables and charts.
Results
Levels of Adolescent and Young Adult Maternal Mortality in Nigeria
Overall, during the period from 1990 to 2017 in Nigeria, a total number of 465,857 maternal deaths occurred in women between the age groups of 1049 years, out of which 122,107 deaths (27%) occurred in adolescent and young women aged 10-24 years. Yearly numbers of adolescent maternal deaths show slight fluctuation from 1990 to 2017, overall showing a slight increase over the time period.
Trends in Adolescent and Young Adult Maternal Mortality in Nigeria
The total number of maternal deaths in the age group of 10-49 years increased steadily from 1990 to 2017, except with fine fluctuations between 2004 and 2013, thereafter increased slightly between 2015 and 2017 (Table 1). For the number of maternal deaths in the age group 10-24 years, there was little fluctuation, ranging from 3,866 (in 1990) to 4,665 (in 2010) (Table 1). Equally, there appear to be fine fluctuations across other measures of maternal mortality. For example, the percent of maternal deaths in the AYA group varied (actually declined) from 29.8% in 1990 to 25.6% in 2017 (a reduction of 3.3%). Similarly, variations in maternal mortality rates and ratios among AYA are fine; for maternal mortality rate, it declined from 592 in 1990 to 423 in 2017 while for maternal mortality ratio, it declined from 26 in 1990 to 13 in 2017. In all these measures, year-to-year variations are very minimal.
| Year | Number of maternal deaths (10-49 years) | Number of maternal deaths (10-24 years) | Percent of maternal deaths aged 10-24 years | MM Ratio* (15-49 years) | MM Rate** (15-49 years) | MM Rate** (10-24 years) | MM Ratio* (10-24 years) |
|---|---|---|---|---|---|---|---|
| 1990 | 12,971 | 3,866 | 29.8% | 322 | 1,725 | 592 | 26 |
| 1991 | 13,370 | 3,975 | 29.7% | 322 | 1,723 | 595 | 26 |
| 1992 | 13,864 | 4,097 | 29.6% | 323 | 1,723 | 596 | 26 |
| 1993 | 14,236 | 4,165 | 29.3% | 322 | 1,720 | 596 | 25 |
| 1994 | 14,700 | 4,253 | 28.9% | 323 | 1,720 | 596 | 25 |
| 1995 | 14,907 | 4,249 | 28.5% | 318 | 1,715 | 594 | 24 |
| 1996 | 15,345 | 4,320 | 28.2% | 317 | 1,687 | 586 | 24 |
| 1997 | 15,644 | 4,346 | 27.8% | 314 | 1,616 | 568 | 24 |
| 1998 | 16,123 | 4,422 | 27.4% | 314 | 1,535 | 546 | 24 |
| 1999 | 16,310 | 4,422 | 27.1% | 309 | 1,464 | 527 | 23 |
| 2000 | 16,561 | 4,436 | 26.8% | 305 | 1,431 | 518 | 22 |
| 2001 | 16,733 | 4432 | 26.5% | 300 | 1,442 | 521 | 22 |
| 2002 | 17,070 | 4,470 | 26.2% | 298 | 1,476 | 526 | 22 |
| 2003 | 17,033 | 4,413 | 25.9% | 290 | 1,519 | 533 | 21 |
| 2004 | 17,068 | 4,393 | 25.7% | 283 | 1,553 | 538 | 20 |
| 2005 | 16,982 | 4,345 | 25.6% | 275 | 1,562 | 537 | 19 |
| 2006 | 17,234 | 4,434 | 25.7% | 273 | 1,550 | 530 | 19 |
| 2007 | 17,561 | 4,517 | 25.7% | 273 | 1,539 | 523 | 19 |
| 2008 | 17,580 | 4,501 | 25.6% | 268 | 1,522 | 515 | 18 |
| 2009 | 17,983 | 4,605 | 25.6% | 268 | 1,506 | 507 | 18 |
| 2010 | 18,250 | 4,665 | 25.6% | 267 | 1,487 | 498 | 18 |
| 2011 | 17,914 | 4,553 | 25.4% | 257 | 1,471 | 491 | 17 |
| 2012 | 17,571 | 4,435 | 25.2% | 248 | 1,457 | 481 | 16 |
| 2013 | 17,196 | 4,308 | 25.1% | 239 | 1,439 | 471 | 15 |
| 2014 | 17,269 | 4,301 | 24.9% | 235 | 1,424 | 459 | 14 |
| 2015 | 17,362 | 4,326 | 24.9% | 232 | 1,406 | 448 | 13 |
| 2016 | 17,603 | 4,407 | 25.0% | 230 | 1,388 | 436 | 13 |
| 2017 | 17,712 | 4,451 | 25.1% | 226 | 1,369 | 423 | 13 |
*Maternal mortality ratio, **Maternal mortality rate
Causes of Adolescent and Young Adult Maternal Mortality in Nigeria
Figures 1 and 2 present the trends in the causes of death in 10-24-year-olds from 1990 to 2017. In Figure 1, sepsis, maternal hypertensive disorder, and obstructed labor are the 3 leading causes of death; these 3 causes are followed by maternal hemorrhage, ectopic pregnancy, and abortion. These trends in rates remained virtually similar across the seven-time points. Sepsis was the main cause of death throughout the period, with a cause-specific MMR of between 168/100,000 live births and 148/100,000 live births; this was followed by maternal hypertensive heart disease as the second leading cause of death with a cause-specific MMR ranging from 165/100,000 live births in 1990 to 120/100,000 live births in 2017, except in 2000 dropping to less than 100/100,000 live births. The third leading cause of death in those aged 10-24 years old was obstructed labor, followed by maternal hemorrhage in the fourth place. Ectopic pregnancy ranked the fifth cause of death, while abortion ranked sixth with an MMR that rose from 3/100,000 live births in 2005 to 8/100,000 live births in 2010.
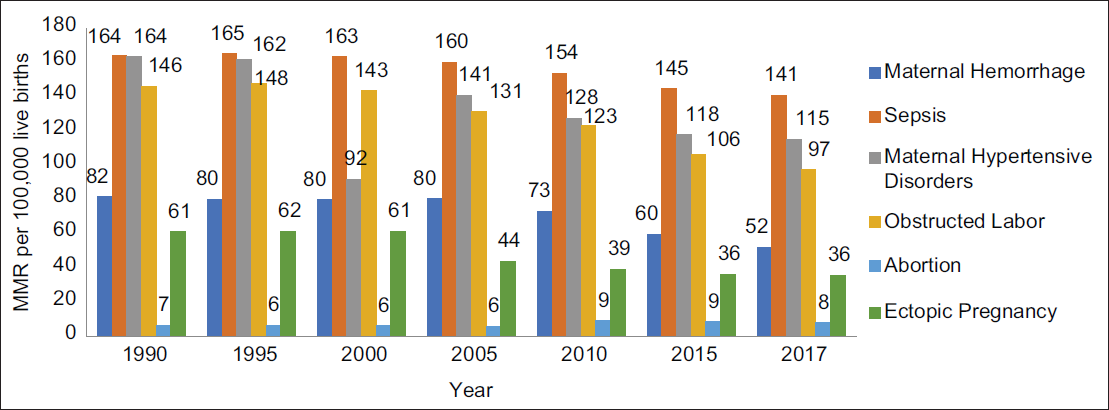
- Trends of the Causes of Adolescents and Young Adults (10-24 years) Maternal Mortality in Nigeria, 1990–2017

- Percentage of Maternal Deaths by Causes in Nigeria, 2017
Figure 2 provides information on the percentage contribution of each of the causes of maternal deaths in the year 2017. The six major causes of death were maternal hemorrhage (41%),abortion (18%),obstructed labor (11%), maternal hypertensive heart disease (8%), and 5% for both sepsis and ectopic pregnancy.
Figure 3 displays the trend of age-specific MMR in Nigeria between 1990 and 2017. This pattern of maternal mortality is consistent with the widely reported J-shaped curve for age-specific maternal mortality (Figure 3). The MMR for adolescents aged 15-19 years was 17% higher than for those young adults aged 20-24 years. Adolescents had a much lower MMR compared to women aged 35 years and older. The trend showed that MMR increased in women aged 30-34 years and peaked in women aged 45-49 years.
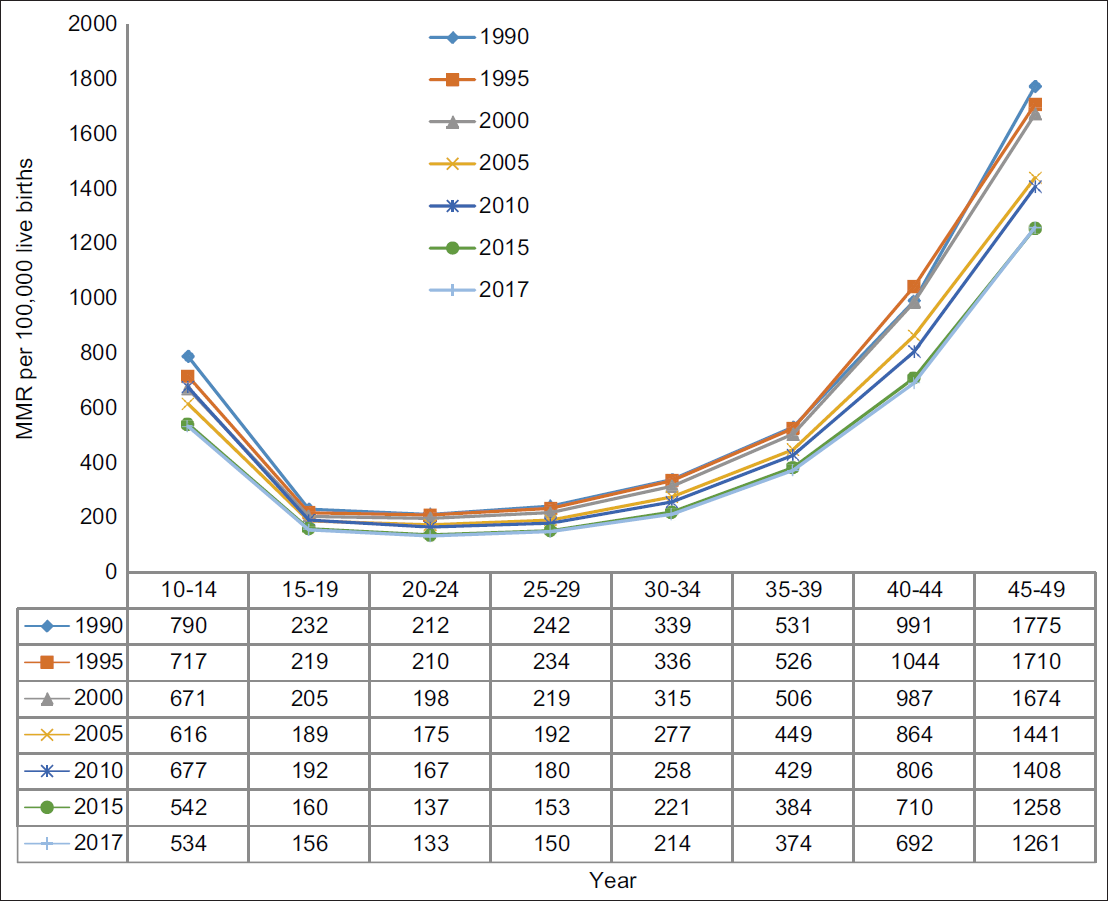
- Age-specifìc Maternal Mortality Ratio in Nigeria (10-49 years), 1990-2017
Discussion
In this study, we sought to determine the levels, changes over time, and causes of adolescent maternal mortality in Nigeria using data available from the GBD Study 2017 provided by IHME. The study revealed that the AYA population contributed between 25% and 30% of maternal deaths in Nigeria. Despite the global progress in the reduction of maternal mortality, the absolute number of maternal deaths among AYA in Nigeria increased progressively between 1990 and 2017, although the proportional contribution to overall maternal deaths showed a decreasing trend. The risk of maternal deaths decreased gradually over the period albeit higher than the figures among women aged 15-49 years.
In terms of the causes of maternal deaths, sepsis, maternal hypertensive disease, obstructed labor, hemorrhage, complications of unsafe abortion, and ectopic pregnancy were the leading causes of death among AYA in Nigeria. These persistently remained major causes of maternal deaths throughout the study period, indicating a need for new ideas and strategies to provide effective solutions to address these preventable public health issues. Studies from other African countries like Ghana, Cameroon, Egypt, and Namibia revealed similar major causes of maternal deaths as in Nigeria.19-22 This underscored the need for multi-pronged innovative strategies at country and regional levels in tackling these causes of adolescent maternal deaths across the continent.23
The causes of maternal deaths highlighted above contrast with previous global reports where maternal hemorrhage, hypertensive disease, sepsis, obstructed labor, and complications of abortion were the leading causes of global maternal deaths.24,25 This difference could, however, be explained by the fact that our study was restricted to adolescents and young adults and not the entire female population. Similar findings from a study conducted in North Central Nigeria corroborated complications arising from unsafe abortion, hypertensive disease (in the form of eclampsia), and sepsis as the leading causes of adolescent maternal deaths.15 Adolescents and young adults are particularly vulnerable to unsafe abortion, especially in countries like Nigeria, where abortion is only allowed by law as an emergency medical intervention to save the lives of the mother. Even then, this service may not be freely available to (especially unmarried) adolescents and young adults because of both family and negative societal attitudes to adolescent pregnancy. These negative attitudes have been associated with a lack of use of maternal and child health services (ANC, skilled delivery, postnatal care, and contraception) by adolescents leading to fatal outcomes such as maternal hemorrhages and obstructed labor.26,27 This study also shows that the indirect causes of maternal mortality are also a challenge in Nigeria, accounting for approximately 8% of maternal mortality. This is similar to the reports of indirect causes of maternal deaths in Bangladesh.28 Indirect obstetric deaths result from previous existing diseases or diseases that developed during pregnancy and are not due to direct obstetric causes but aggravated by the physiologic effects of pregnancy.29
The age-specific MMR among AYA in this study revealed a similar picture to the previously reported classical J-shaped curve.1 As shown in Figure 3, among the AYA, the MMR was highest in the age group 10-14 years, decreasing to the lowest in those aged 20-24 years before making a smooth climb to peak among those aged 45-49 years. Thus, highlighting that the risk for maternal death was higher at the extreme of this age group. Oliveira et al. and Yogev et al. similarly reported severe maternal morbidities and fetal risk at the older clime of the reproductive age group.29,30
Conclusion and Implications for Translation
This study shows that AYA are at increased risk of maternal deaths in Nigeria. The majority of the deaths are due to sepsis, maternal hypertensive disease, obstructed labor, hemorrhage, and complications of unsafe abortion. Therefore, maternal health programs in Nigeria need to have a specific program that targets the AYA for the prevention of and reduction of incidences of maternal death among this population group in the country. Programs should specifically focus on preventing the major causes of AYA mortality elicited. The study findings highlight the need for adolescent-friendly health services that provide AYA with all elements of care ranging from before pregnancy through pregnancy, childbirth, and the postpartum period. It is critical to advocate for policymakers for adequate implementation of adolescent health policies at national and subnational levels.
Compliance with Ethical Standards
Conflicts of Interest:
The authors have no conflicts of interest to disclose.
Financial Disclosure:
The authors have no relevant financial interests to disclose.
Ethics Approval:
This study was a secondary analysis of publicly available data; therefore, no institutional review board was required.
Disclaimer:
None.
Acknowledgments:
None.
Funding/Support:
No funding was received for conducting this study.
References
- Millennium development goal 5 and adolescents: looking back, moving forward. Arch Dis Child. 2015;100(Suppl 1):s43-s47.
- [CrossRef] [PubMed] [Google Scholar]
- Trends in Maternal Mortality: 1990 to 2017: Estimates by WHO, UNICEF, UNFPA, World Bank and the United Nations Population Division. Geneva: World Health Organization; 2019.
- [Google Scholar]
- Health of the world's adolescents: a synthesis of internationally comparable data. Lancet. 2012;379(9826):1665-75.
- [CrossRef] [PubMed] [Google Scholar]
- United Nations, Department of Economic and Social Affairs, Population Division. In: World Population Prospects 2019. New York: United Nations; 2019.
- [Google Scholar]
- Growing Up Global: The Changing Transitions to Adulthood in Developing Countries. Washington DC: National Academies Press; 2005.
- Adolescent health programs. In: Jamison DT, Breman JG, Measham AR, eds. Disease Control Priorities in Developing Countries. Washington DC: World Bank; 2006. p. :1109-1125.
- [CrossRef] [Google Scholar]
- 2008. The Global Burden of Disease: 2004 Update. World Health Organization; (accessed )
- State of the World's Children: Celebrating 20 Years of the Convention on the Rights of the Child. UNICEF; 2009.
- [Google Scholar]
- Commission on Population and Development: Report on the Forty-Fifth Session.Economic and Social Council Official Records, 2014. 2012.
- Maternal mortality in adolescents compared with women of other ages: evidence from 144 countries. Lancet Glob Health. 2014;2(3):e155-164.
- [CrossRef] [PubMed] [Google Scholar]
- New Findings for maternal mortality age patterns: aggregated results for 38 countries. PLoS One. 2013;8(4):e59864.
- [CrossRef] [PubMed] [Google Scholar]
- Adolescent Maternal Mortality in North-west Nigeria. West Afr J Med. 2012;31(4):224-226.
- [Google Scholar]
- Obstetric outcome of teenage pregnancies at a tertiary care hospital in Sokoto Nigeria. Trop J Obstet Gynaecol. 2005;22:168-70.
- [CrossRef] [Google Scholar]
- Adolescent maternal mortality in Sokoto Nigeria. J Obstet Gynaecol. 2003;23(2):163-5.
- [CrossRef] [PubMed] [Google Scholar]
- Maternal mortality among adolescent women in Jos, north-central, Nigeria. J of Obstet Gynaecol. 2005;25(1):3-6.
- [CrossRef] [PubMed] [Google Scholar]
- Frequently Asked Questions. (accessed )
- Institute for Health Metrics and Evaluation. 2018. Global Burden of Disease Study 2017 (GBD 2017) Results. IHME, GHDx; (accessed )
- [Google Scholar]
- Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1736-88.
- [CrossRef] [Google Scholar]
- Distribution of causes of maternal mortality among different socio-demographic groups in Ghana; a descriptive study. BMC Public Health. 2011;11(1):159.
- [CrossRef] [PubMed] [Google Scholar]
- Maternal mortality in Cameroon: a university teaching hospital report. Pan Afr Med J. 2015;21(1):16.
- [CrossRef] [Google Scholar]
- Maternal mortality in Giza, Egypt: magnitude, causes, and prevention. Stud Fam Plann. 1992;23(1):45-57.
- [CrossRef] [PubMed] [Google Scholar]
- Maternal, fetal, and neonatal outcomes associated with measles during pregnancy: Namibia, 2009-2010. Clin Infect Dis. 2014;58(8):1086-92.
- [CrossRef] [PubMed] [Google Scholar]
- Factors associated with maternal mortality in Sub-Saharan Africa: an ecological study. BMC Pub Health. 2009;9(1):462.
- [CrossRef] [PubMed] [Google Scholar]
- Maternal mortality: who, when, where, and why. Lancet. 2006;368(9542):1189-200.
- [CrossRef] [PubMed] [Google Scholar]
- WHO analysis of causes of maternal death: a systematic review. Lancet. 2006;367(9516):1066-74.
- [CrossRef] [PubMed] [Google Scholar]
- Young people's perception of sexual and reproductive health services in Kenya. BMC Health Serv Res. 2014;14:172.
- [CrossRef] [PubMed] [Google Scholar]
- Barriers to accessing maternal health care amongst pregnant adolescents in South Africa: a qualitative study. Int J Pub Health. 2020;65(4):469-76.
- [CrossRef] [PubMed] [Google Scholar]
- Indirect causes of maternal death. Lancet Glob Health. 2014;2(10):e556.
- [CrossRef] [PubMed] [Google Scholar]
- Severe maternal morbidity and maternal near miss in the extremes of reproductive age: results from a national cross-sectional multicenter study. BMC Pregnancy Childbirth. 2014;14(1):77.
- [CrossRef] [PubMed] [Google Scholar]
- Pregnancy outcome at extremely advanced maternal age. Am J Obstet Gynecol. 2010;203(6):558-e1-7.
- [CrossRef] [PubMed] [Google Scholar]



