

Translate this page into:
Polio Eradication in Nigeria and India: A Systematic Review of Challenges and Successes
Abstract
Background:
The global eradication of polio is considered an emergency and an unaccomplished task until completely eliminated. Vaccinating children against the polio virus confers immunity on them and breaks the transmission of the polio virus. Afghanistan, Nigeria and Pakistan remain the only three countries in the world that have not eliminated polio. The aims of this paper were to: (1) to identify the factors that impact the failure to eliminate polio from Nigeria and (2) determine the factors that led to the successful elimination of polio from India.
Methods:
A systematic literature review was carried out to meet the above research objectives. Four electronic databases were searched (Cochrane Library, Medline, PubMed and Google Scholar) and articles that fulfilled the inclusion and exclusion criteria were selected and critically appraised.
Results:
In all, 98 articles were retrieved. After selection based on our selection criteria, fourteen studies were identified and included in the study. These were 5 systematic reviews: 3 cross-sectional studies, 3 mixed methods studies, 2 case-control studies and one quantitative (survey) study. In all, seven themes were identified from the review of the articles. Four themes were identified from the factors associated with the failure to eliminate polio from Nigeria: (1) Failure of the oral polio vaccine (OPV); (2) Institutional and geographical failures in vaccine programs; (3) Program and campaign management limitations; and (4) Vaccine refusal. Similarly, three themes were identified from the factors that contributed to the elimination of polio from India: (1) Replacement of the trivalent OPV with the monovalent and bivalent OPVs; (2) Implementation of intensive social mobilization strategies; and (3) Effective program micro planning and campaign management.
Conclusion and Implications for Translation:
Based on the findings from the literature review, we highlight areas where Nigeria can learn from India in its quest to eliminate polio. These factors can form the basis for future theoretical and policy reforms in the fight against polio not only in Nigeria but in countries where it remains endemic. Further research should compare the success of polio eradication in other countries.
Keywords
Polio
Immunization
Nigeria
India
Pakistan
Eradication
Systematic Review

Introduction
Since the early 20th century, polio has been one disease that has caused permanent disability and death to thousands of children.1 Polio has a history that dates to ancient times, but it was not until 1789 that British physician Michael Underwood described the clinical syndromes of the disease.2
Polio, also known as poliomyelitis or infantile paralysis, is an infectious disease caused by the polio virus.3 Poliomyelitis is derived from two Greek words; ‘polio’ and ‘myelitis’. Polio is translated as ‘grey’, while ‘myelitis’ is from the word ‘myelon’ which refers to the marrow of the spinal cord. In general usage, the term ‘poliomyelitis’ is shortened to ‘polio’. Polio typically affects the spinal cord producing its classical symptoms of paralysis.4
When given appropriately, vaccines prevent polio and protect the recipient for life.5 Through the Expanded Program on Immunization (EPI), the World Health Organisation (WHO) recommends 4 doses of the oral polio vaccine (OPV) for children at birth, 6, 10 and 14 weeks.5 However, in conditions where spread of polio virus is enhanced (due to hot weather or poor hygiene), more than four doses of the OPV can be administered.5 There are broadly two types of polio vaccine, the inactivated polio vaccine and the weakened oral polio vaccine.4 These two types are active as follows: the inactivated polio vaccine (IPV) protects against poliovirus types 1, 2 and 3; the trivalent OPV protects against poliovirus types 1, 2 and 3; the bivalent OPV protects against poliovirus types 1 and 3; while the monovalent oral polio vaccines 1 and 3 (mOPV1 and mOPV3) protect against poliovirus types 1 and 3 respectively.5
Disease elimination and eradication are often interchangeably used. Although both terms are commonly used, public health concepts are different. While disease elimination is the reduction to zero of the number of new disease or infection cases within a defined geographical region, disease eradication is a global and permanent reduction to zero of a disease or infection.6
The world has never been this close to eradicating polio.7 However, for its eradication to be complete, no country must be left out.8 In the recent past, polio has made a comeback, arising principally from countries where the transmission of the wild polio virus has not been interrupted.9 Failure of global efforts to eradicate polio could result in thousands of children being re-infected with resulting paralysis and huge financial burdens; failure could also endanger immunization efforts around the world thereby putting the lives of thousands of children at risk.7
The eradication of poliomyelitis is a public health emergency,10 and the elimination of polio virus from endemic countries is central to its eradication.11 Any child that is not vaccinated against polio remains a threat to other children in the world, and unless every child is vaccinated, its transmission cannot be broken.5 When a large proportion of children in a given population are vaccinated against polio, community or herd immunity can be achieved in the population.12 Herd immunity confers immunity to unvaccinated or to children/individuals in whom vaccination is contraindicated; it reduces the probability that those not immune/vaccinated from the disease will come in contact with infected individuals.12 For effective herd immunity, 80 – 85% of children within a community need to be vaccinated. However, a fall in the number of vaccinated individuals in the community reduces the potency of herd immunity, and unvaccinated individuals are at risk of being infected by the polio virus.13
Despite the polio virus not being globally eradicated, there has been progress from when efforts towards eradication began in 1988. During this time, polio was endemic in at least 125 countries with an estimated 350,0 individuals paralyzed by the disease.14,15,1 In a turn of fortunes, only 359 cases were detected globally in 2014 and these cases were concentrated in Afghanistan, India and Nigeria.11
Up until 2015, Nigeria was one of the only remaining countries in the triangle of countries that were still susceptible to the transmission of the wild polio virus.15 Nigeria was declared polio-free in September 2015 by the WHO.15 However one year later, a wild polio virus case was detected. No wild polio virus was detected in 2017 while there have been a few cases of vaccine-derived infections detected in 2018 and 2019. In 2012, India was declared polio-free by the WHO.16 It is important that the transmission of polio is interrupted; achieving this goal would get the world closer to total eradication of polio.17
Rationale for the study
Polio is a highly contagious disease which mainly affects children under the age of five years.5 It is responsible for causing life-long paralysis in thousands of victims, as well as deaths from complications of the disease.5 It is a public health emergency because of the long-term disability it causes and the risk it poses to every child around the world until it is eradicated everywhere.7
In the recent past, polio has made a comeback, arising principally from countries where the transmission of the wild polio virus has not been interrupted.9 Failure of global efforts to eradicate polio could result in thousands of children being re-infected with resulting paralysis and huge financial burdens; failure could also endanger immunisation efforts around the world thereby putting the lives of thousands of children at risk.7
Although no known previous studies comparing the respective efforts of Nigeria and India has been published, a few studies have been carried out which look at the dynamics and challenges of polio eradication in both countries. The Expanded Program on Immunization (EPI) was introduced in India in 1978 and had a limited reach to mostly urban populations. Then, in 1985, India launched the Universal Immunization Program which had an improved and phased implementation drive; local capacity was also enhanced. Prior to the 1990's, India was the worst hit among developing countries by polio.16 India's real efforts at eliminating polio commenced in the years 1995 – 1996, spearheaded by the Global Polio Eradication Initiative (GPEI) and the WHO and supported by the Centre for Disease Control (CDC), Rotary international, and UNICEF: This gave rise to the National Polio Surveillance Project.16 By January 13th 2011, the last case of the wild polio virus in India was reported and in 2014 the country was certified polio free by the WHO.16
Nigeria launched the EPI in 1979 and by the 1980's there were a few advances that were made with up to 80% coverage in the years 1986 – 1990. This was followed by a sharp decline in the 1990's.17,18 In 1997 the Federal government of Nigeria restructured and centralized the EPI and renamed it the National Program on Immunization (NPI). The (Nigerian) National primary health care development agency (NPHCDA) was merged with the NPI in 2007 following a general health sector reform by the Federal government of Nigeria. The primary mandate of the NPHCDA is to protect children from vaccine-preventable diseases through the provision of vaccine, technical organization and general mobilization of the populace.18
The global fight against polio was threatened in 2003 when communities in Northern Nigeria rejected polio immunization due to rumors spread and supported by local Muslim clerics about the oral polio vaccine (OPV), alleging that the vaccine made children sterile. This resulted in multiple states in the northern part of the country completely missing polio vaccination in children.17 The result was a massive outbreak in Nigeria and a spread to other previously polio-free African countries and parts of the Middle East. This was the first time it had happened at that stage of the polio eradication efforts and meant that gains made in eradicating polio from those countries had been rolled back.19
Research objectives
The objectives of this were study were to: (1) identify factors that have contributed to the failure/delay in eradicating polio in Nigeria; (2) determine factors that have influenced the success of eradicating polio in India; and (3) comparatively evaluate factors in objectives one and two above. Our aim was to analyze the factors that have influenced the eradication of polio in India and Nigeria. Now that Nigeria has successfully eradicated polio by using multiple approaches, lessons learned from India's success story are still pertinent not only for Nigeria but for other polio endemic countries and for the planning and implementation of other populations-based public health programs.
Methods
A systematic literature review was carried out to meet the aim and objectives of the study.
Search strategy
A systematic literature search was conducted in the following electronic databases; PubMed, Medline, Google Scholar and Cochrane library. The period between 2006 to 2016 was covered. The search for articles included the use of expanded MeSH headings and keywords combined using Boolean operators (‘AND’ and ‘OR’) on these terms: perspectives, polio, eradication, Nigeria, India, comparative, and evaluation.
The reference section of included articles was also manually searched for relevant articles.
Study selection
Studies included in the study were primary and secondary research on polio in India and/or Nigeria, were written in English, and were conducted from 2006 - 2016.
Data extraction: Summary Tables
Data was extracted using a modified version of the guidelines used by the Centre for Reviews and Dissemination.19 The modified data extraction form includes information such as the title of article, author, type of study, and journal type/information. It also includes study characteristics such as the aims and objectives of the study, study design, study population/population characteristics, results of the study, outcome of the study, source of funding, ethical considerations, and location of the study.
Before data extraction, the data extraction form was tested on a few of the articles to ensure that the form contained all relevant information applicable to the study.
Data analysis
A thematic analysis was used to analyze data from the study. Once results were collated and appraised, common themes and variations were identified and arranged. Thematic analysis involves the identification, evaluation and documenting of patterns or themes.20 Themes are described as patterns or reoccurrences of similar information which describe phenomenon and are associated with the answer(s) to a research question.20 Thematic analysis is not confined to particular types of studies and can be used in systematic literature reviews.20 The use of mind maps was employed to further enhance the quality of the thematic analysis. The themes were presented in two separate tables lettered A – G, with A – D representing themes from studies on Nigeria while E – G represents themes derived from studies on India. A matrix of the themes A – G derived from the studies was drawn.
Six steps were used to carry out the thematic analysis: (1) data were collected and gathered, while patterns were established following iterative reading of the literature; (2) initial codes for the data were generated; (3) collation of the data from the codes developed in step two; (4) themes were identified; (5) themes were defined; and (6) the findings were reported.
Quality of included studies
Studies that met the inclusion criteria were critically appraised using the Evaluation Tool for Quantitative Research Studies by Long et al.21 and Critical Appraisal Skills Program (CASP) tools for research appraisal.22 The framework for critical appraisal was dependent on the study design of the article.
Ethical considerations
There was no requirement for ethical approval as secondary data was used in this study. However, primary studies that were included in the review were screened for their respective ethics approvals. Studies that did not meet ethical standards were not included.
Results
Search for literature yielded 3,267 articles. Removal of duplications, title and abstract screening narrowed the number to 219 articles. Twenty-seven articles were unavailable while 178 articles were further excluded based on the inclusion criteria. Figure 1 shows an adapted PRISMA diagram of the study selection process.
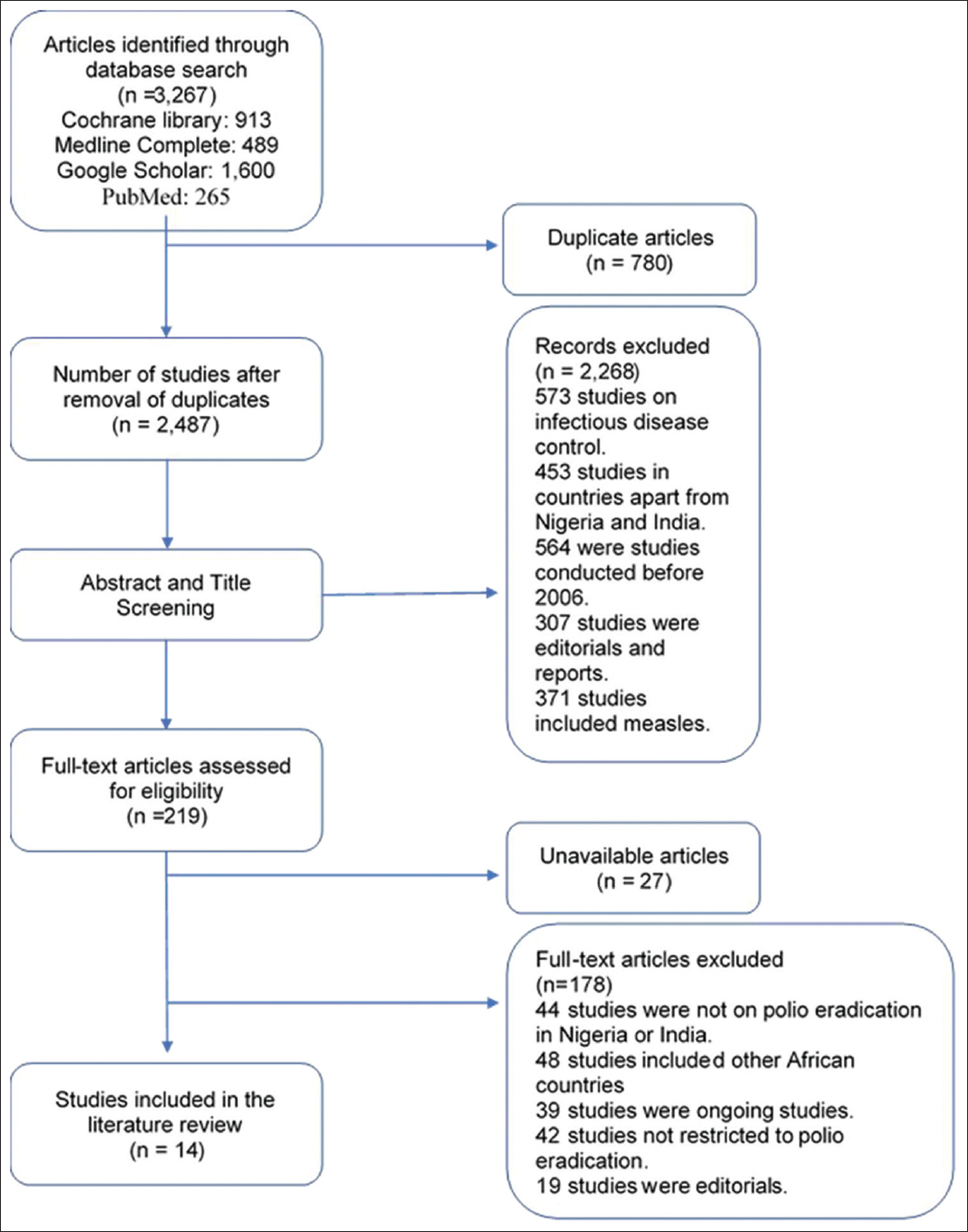
- PRISMA diagram flowchart of search results
Summary of findings
Although there are no specific studies that have been reported to compare Nigeria and India in relation to the fight against polio, a few overlapping factors have been identified in the challenges facing both countries.
India was chosen as a country of comparison because of the similar socio-demographic factors it shares with Nigeria. More importantly because it is one of the last major countries that still had the polio epidemic and has since eliminated the disease.23 Since 2012, Nigeria has been the primary source of all wild polio virus that has surfaced in polio-free countries of Africa and even in Asia.14 The researchers identified major themes that have limited the fight against polio in Nigeria. These include (a) failure of the polio vaccine, (b) outright refusal of the vaccine, (c) insecurity and institutional challenges, and (d) limitations to the vaccine and campaign program management. Factors that have contributed to the successful eradication of polio in India include (a) the replacement of the type two containing trivalent OPV with the mono and bivalent OPV (b) massive social mobilization strategies, and (c) effective macro and micro planning of vaccine campaigns.
Factors in the failure of polio eradication in Nigeria
Failure of the oral polio vaccine has been implicated in the resurgence of polio and its eradication failure from Nigeria.24,10 These failures have been ascribed to the use of the type 2 trivalent OPV, which is currently being replaced by the mono and bivalent OPV24,10 Malnutrition, poor sanitation and under-immunized or non-immunized children have also been factors in the failure of the polio vaccine.10 This is also linked to the circulating-vaccine derived polio virus 2 (cVDPV2). Although it has a low incidence rate, this form of the vaccine derived virus does result in paralysis and has been responsible for acute flaccid paralysis in Nigeria.25 The surveillance team may be confounded by this type of paralysis and may assume the transmission is an outbreak. Likewise, the process may cause local communities to increase their skepticism of the polio vaccine.26 In 2003, refusal of the polio vaccine by some communities in Northern Nigeria resulted in a global outbreak of the wild polio virus.14 This refusal of child vaccination originates from cultural and religious beliefs as well as from false rumors, such as the belief that vaccines contain substances that sterilize populations. 27,30,10 Vaccine refusal has also been linked to a lack of trust within vaccination teams.11 This lack of trust can be attributed to knowledge gaps, illiteracy, and socio-political dynamics among religious clerics in the affected regions.11
A severe limitation in the fight against polio in Nigeria has been the challenge of the vaccine campaign management and implementation of policies. There have been instances of poorly trained and poorly motivated staff/local officials11 with the attendant consequences, such as missed vaccinations in children, outright failure to vaccinate children and poor communication with care-givers.26,29 Without the local staff's commitment to polio mitigation, the aims and goals of the vaccination programs may not be met. Furthermore, there has been poor accountability and data management of acute flaccid paralysis in children28 and in some cases, the outright failure of household visitations by vaccine/local officials.29 This deficiency can be linked to negligence by supervisory officials of vaccine campaigns.27
Institutional factors, insecurity and geographically difficult terrain are potent factors in the failure of polio eradication in Nigeria. There is a general trend of distrust among the local populations stretching across Northern Nigeria.10 Michael et al.29 have also mentioned how ignorance of the vaccine and its physical absence have contributed to a failure of the vaccination drive. Communities in the north-eastern corner of Nigeria are ravaged by insecurity, with a brutal insurgency going on; children have limited access to vaccination as a result of these insecurity challenges.27 Steelfisher et al.11 mentioned there is a marked difference between those in conflict areas and those that have limited access to vaccination.
Factors pertaining to successful eradication of polio in India
Effective vaccination has been central to the eradication of polio from India. Bahl et al.30 observed that the use of the trivalent OPV was less effective than the mono and bivalent OPV's in India. Some of these effects appeared to be affected by the nutrition status of children being administered the vaccines. Deshpande et al.31 however recommended that the monovalent OPV be used along with intermittent doses of the trivalent vaccine. What is obvious from this is that the trivalent vaccine is less effective than the mono and bivalent vaccines. This view is supported by the WHO which has commenced a gradual program of replacing the trivalent OPV's with the bivalent OPV5 However, this may also be explained by the Hawthorne effect. According to this theory, any new intervention might cause a temporary positive effect and would eventually wear off.32
India is the second most populous country in the world and without effective and massive social mobilizations, vaccination of a vulnerable population would be a daunting task. One major factor that has contributed to the successful elimination of polio from India has been the intensive social mobilization. This was mostly achieved through the social mobilization network (SMNet) and Core Group Polio Project (CGPP); effective vaccination has also been achieved by orientation campaigns that have been used to disabuse the minds of caregivers from the negative campaigns against the polio vaccine.33 The challenge of earning the trust of key social and religious leaders was achieved through local community mobilization.34 The strategy was also important in providing for the local needs of marginalized communities,34 which also involved government interventions.36,1 The challenge of missed children during immunizations was surmounted by the concept of biphasic vaccinations which involved second teams of vaccinators visiting households where there were missed children and convincing the caregivers to allow their children to be vaccinated.34 Transit vaccination of children in public places such as motor parks, train stations and markets was also employed, in addition to national immunization days done at immunization booths.16
In collaboration with international organizations (United Nations Children's Fund (UNICEF), CORE Group Polio Project (CGPP) and Rotary United), effective micro-planning of vaccine campaigns laid the foundation for an effective polio eradication drive in India.34 To ensure prompt reporting of new cases of paralysis cases in children, active surveillance structures were put in place.36,18 The fight against polio was taken as a matter of national pride1 and vaccinators and local officials were effectively trained and re-trained with national patriotic sentiments ignited, all in a bid to squarely face the menace of polio.34
Discussion
Analysis of results
A thematic analysis was used to analyze data gathered from the search of articles using 3 steps: (1) line by line coding of article text; (2) creation of mind maps; and (3) the development of themes and subthemes. Figures 2 and 3 are mind maps illustrating the factors that have respectively impeded the eradication of polio in Nigeria and factors that contributed to the successful eradication of polio in India. Tables 1 and 2 are themes derived from included articles describing factors responsible for the failure to eradicate polio and factors that supported polio eradication in Nigeria and India, respectively.
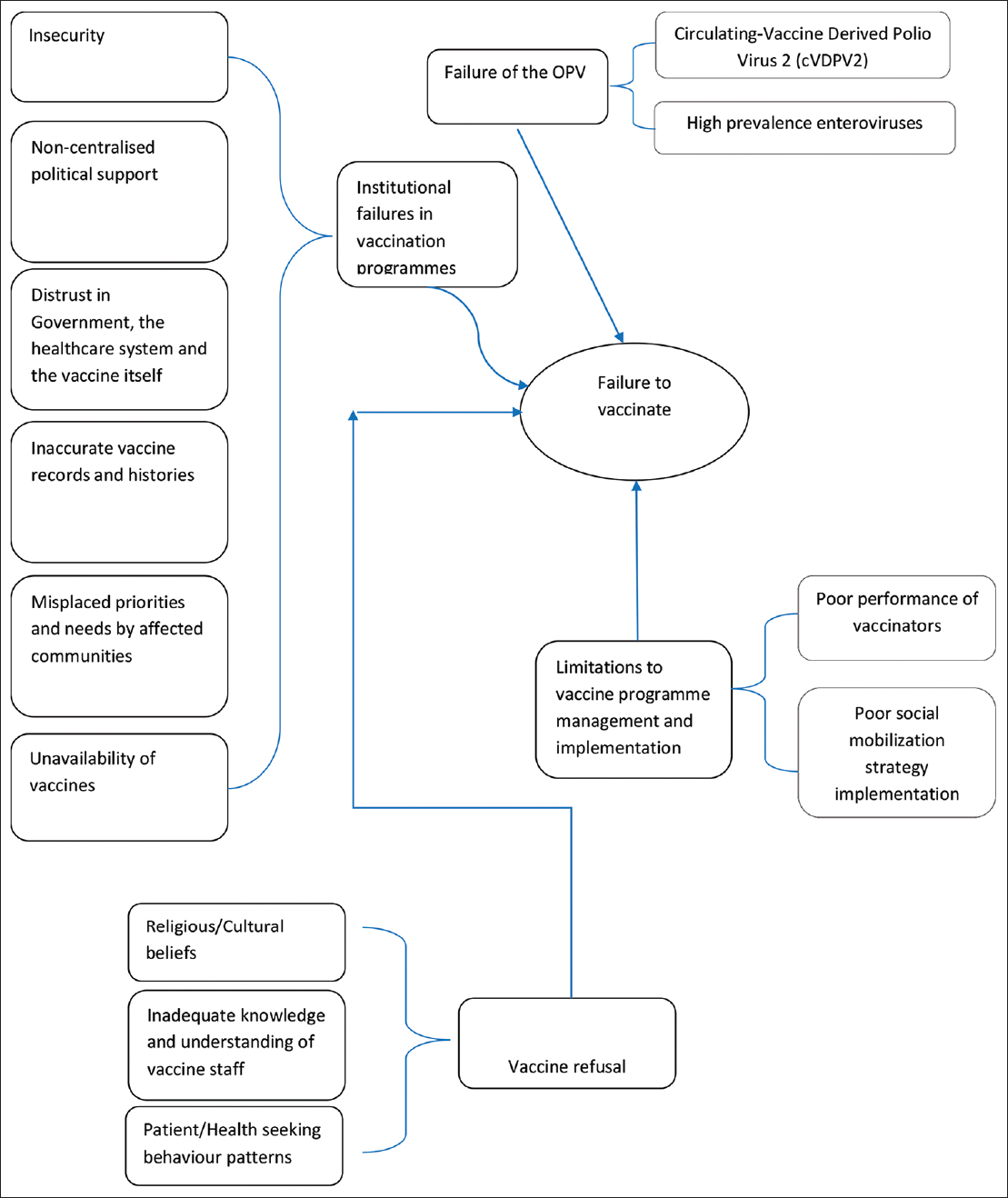
- A mind map showing factors that contributed to the failure to eliminate polio in Nigeria
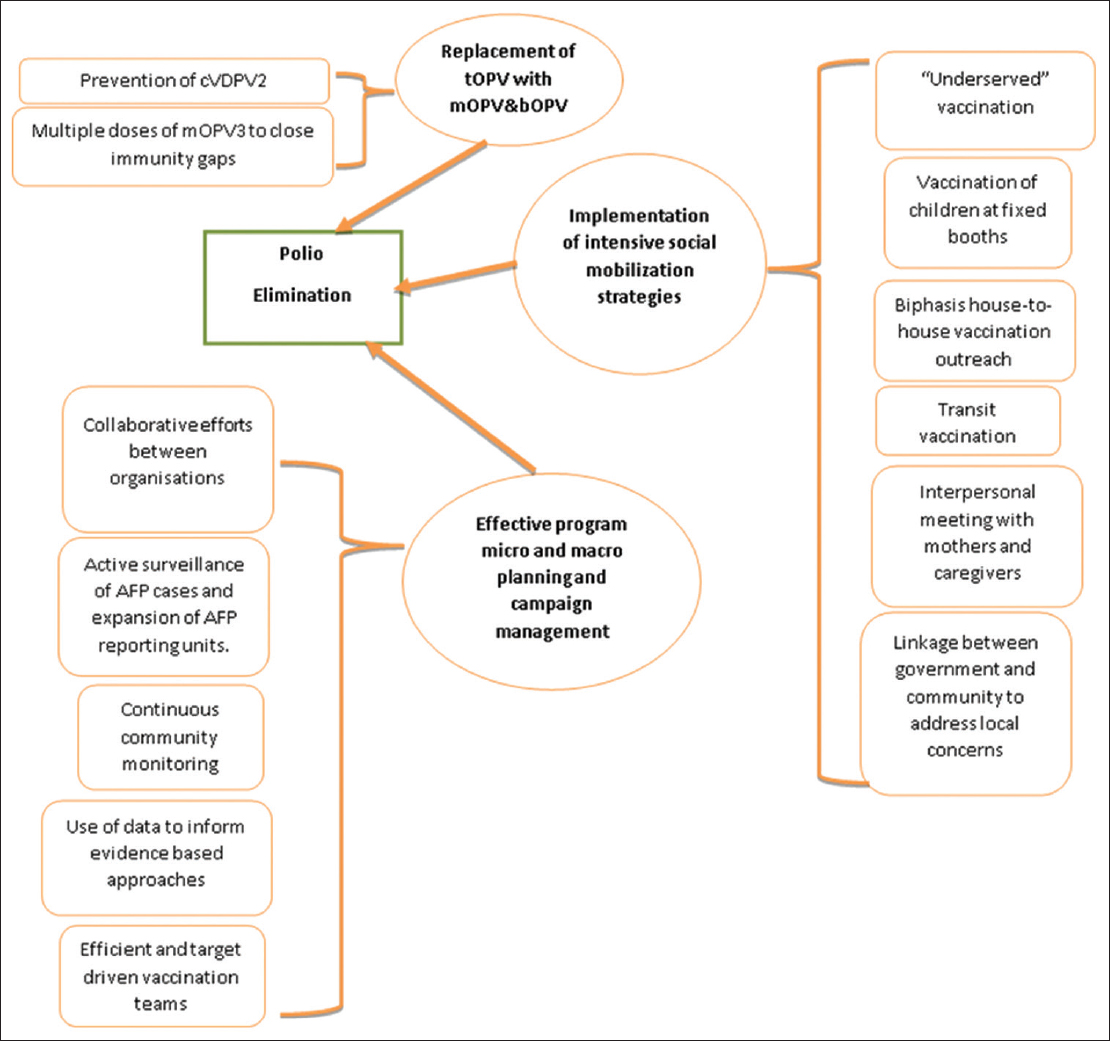
- A mind map showing the factors that contributed to the successful elimination of polio in India
| Theme A Failure of OPV | Theme B Institutional & Geographical failures in vaccine programs | Theme C Program and Campaign Management Limitations | Theme D Vaccine Refusal |
|---|---|---|---|
| 1. Incidence of circulating-Vaccine Derived Polio Virus 2 (cVDPV2). 2. High prevalence of enteroviruses in northern Nigeria might cause lower efficacy of OPV. |
1. Insecurity. 2. Heterogeneous political support. 3. Lack of trust of the people in the healthcare system and government. 4. Unavailability of vaccines/lack of access. 5. Inaccurate vaccine histories and records. 6. Other priorities of needs and wants by the community from government. |
1. Knowledge gap and poor performance of vaccination teams. 2. Inaccurate vaccination histories. 3. Poor implementation of community social mobilization strategies. |
1. Religious beliefs. 2. Cultural beliefs and limitations. 3. Rumors. 4. Knowledge gap of caregivers, mothers/heads of households. 5. Poor health seeking behavior. 6. Absence of child at home. 7. Polio not seen as a priority concern. 8. Lack of tertiary education. |
| Theme E Replacement of tOPV with mOPV and bOPV | Theme F Implementation of intensive social mobilization strategies | Theme G Effective program micro planning and campaign management |
|---|---|---|
| 1. Prevention of incidence of cVDPV2. 2. Multiple doses of mOPV3 to close immunity gaps to type 3 polio in “underserved” areas with high prevalence of malnutrition. 3. mOPV and bOPV more effective than tOPV. |
1. Biphasis house-house vaccination outreach. 2. Community Mobilization Coordinators (CMCs) consist of mostly women. 3. Interpersonal communication meeting with mothers and caregivers. 4. Meetings with mothers of children up to 5 year of age. 5. Linkage between government and community to address local concerns. 6. Vaccination of children at fixed booths. 7. “Underserved” strategy. 8. Transit vaccination strategy. 9. Aggressive campaign. |
1. Collaborative effort between organizations (UNICEF, CGPP, Rotary United) and local government. 2. “War on polio” mentality. 3. Efficient and target driven vaccination teams through application of human resource strategies. 4. Active surveillance of Acute Flaccid Paralysis (AFP) cases and expansion of AFP reporting units. 5. Continuous community monitoring. 6. Use of data to inform evidence-based approaches. |
Comparing the two countries
From a critical perspective, there are several lessons and strategies Nigeria can learn and adapt from the successful approach to polio eradication that was adopted in India. There are minimal differences between the strategies and local conditions of both countries. In contrast, India has the determination of the government and stakeholders in implementing strategies, despite the adverse odds of achieving elimination. Poor performance of vaccination teams, insecurity and a potent refusal for vaccines seem to be the major challenges in Nigeria. India's vaccination teams were more effective, perhaps due to India's measures to motivate and provide a suitable work environment for vaccinators. The insecurity challenges faced in northern Nigeria as a result of the Boko-Haram insurgency were not a problem in India at the time of their vaccination campaign. The insecurity problem might have affected the productivity of the vaccination teams and the monitoring of vaccination activities. Insecurity has also caused mass displacement of populations; program coordinators were presented with massive logistical nightmares. Nevertheless, this insecurity does not justify issues, such as inaccurate vaccination histories, records and poor attitude of vaccinators, these need to be addressed.10
Vaccine refusal, a major challenge in Nigeria, was successfully overcome in India by homogenous political support and aggressive implementation of social mobilization strategies. Efforts should be made in Nigeria to gain the trust of key informants, market heads, and religious and cultural leaders, as it seems the people would rather listen to leaders who they can relate to rather than the government. The government should also make efforts to address other children's health issues that are of concern to people, including the provision of clean drinking water and basic health care infrastructure. The refusal of citizens to vaccinate their children might just be a way to get the government's attention on issues that concern citizens the most, as they have seen the program's importance to the government.26 Thus, the importance of government and healthcare officials in earning the people's trust cannot be exaggerated; it is imperative that officials provide much more than just routine vaccinations to populations of vulnerable children. Government officials can also legislate and implement laws that make vaccination refusal of children an offence that is punishable with prosecution of the offending parents/guardians. This practice is normal in countries such as Pakistan; but the success of that approach has not been proven.35 However, mandatory vaccination has been shown to greatly reduce infection rates for certain diseases worldwide.36 Successful polio immunization has other benefits among which is the ease in which vaccines for other infectious diseases can also be effectively delivered.
Conclusion and Implications for Translation
Insecurity, difficult geographical terrain, negative publicity about the polio vaccine, vaccine failure, rejection of the vaccine, faulty vaccine campaign management, and poorly trained and motivated vaccination staff have all contributed to the failure of polio eradication from Nigeria. On the other hand, replacement of the trivalent oral polio vaccine with mono and bi-valent vaccines, effective social mobilization, and detailed vaccine campaign micro planning have contributed to the successful eradication of polio from India. Both countries have lessons to learn from polio eradication activities to completely eradicate the disease (Nigeria) and to prevent resurgence of the disease (India).
Theoretical and policy implications
The difference in policy and implementation which form the basis for the comparison of the factors for and against the eradication of polio from Nigeria and India need to be revisited. This is to enable further research to find applicable and practical factors in favor of polio eradication. Policy interventions by stakeholders need to be re-examined and juxtaposed with current best practice and up-to-date strategies. The replacement of the trivalent OPV with the mono and bivalent OPV has been shown to have a greater efficacy with polio eradication. Involving local communities and conducting second sweeps during vaccination campaigns have proven to be effective in India. The strategy of vaccinating children in India at transit points is a novel approach that provides another layer to capture children who may have been missed in vaccination campaigns. This strategy, if adopted, can be used to support the desire for an increased surveillance coverage assessment of polio vaccination in Nigeria.
Limitations of the study
There is a moderate to high risk of bias in most of the included studies as none of them was a Randomized Control Trial (RCT). All the other study designs had varying degrees of increased bias as there was the absence of random allocation of interventions and inadequate blinding.
Considering that research on polio eradication in Nigeria and India are linguistically not restricted to English, there is the potential bias that important papers in other languages may have been missed in the review. There is also a chance of selective reporting bias by this researcher as interpretation of findings from included findings were subject to the understanding of the researcher and may have misrepresented the respective authors' intentions. This was mitigated by a transparent adherence to the protocol of the study and a detailed summary table reporting outcomes of respective studies.
India and Nigeria are diverse and heterogenous. It is possible that interventions/studies carried out in sections of both countries might not be feasible or generalized in other parts of the respective countries. Similarly, interventions in urban centers may be of totally different contexts to rural areas.
Compliance with Ethical Standards
Conflict of interest:
The authors have no conflict of interest.
Financial Disclosure:
Nothing to declare.
Ethics Approval:
Ethics approval was not applied for considering no human subjects were involved in this study.
Disclaimer:
None.
Acknowledgments:
I am most grateful to my MSc supervisor, Jane Goodman-Brown, whose understanding, generous support and unwavering guidance made it possible for me to work on a topic of great interest to me. It was a pleasure working with her.
Funding/Support:
The author(s) received no specific funding for this work.
References
- 2015. History of Polio. (accessed )
- Polio's Legacy: An Oral History. University Press of America; 1996.
- Epidemiology and Prevention of Vaccine-Preventable Diseases (12th). Centers for Disease Control and Prevention; 2011.
- 2015. Poliomyelitis. (accessed )
- About the polio end game strategic plan 2016. (accessed )
- The principles of disease elimination and eradication. Bull World Health Organ. 1998;76(suppl 2):22-25.
- [Google Scholar]
- Action to Stop Polio Now in Nigeria, Pakistan, and Afghanistan. 2013. 2012. Global Polio Emergency Plan 2012-2013. Geneva: WHO; (accessed )
- [Google Scholar]
- Making history: from a public health emergency to a polio-free world. Bull World Health Organ. 2014;92(7):466.
- [CrossRef] [Google Scholar]
- Key issues in the persistence of poliomyelitis in Nigeria: a case- control study. Lancet Glob Health. 2014;2(2):e90-e97.
- [CrossRef] [Google Scholar]
- Threats to polio eradication in high-conflict areas in Pakistan and Nigeria: a polling study of caregivers of children younger than 5 years. Lancet Infect Dis. 2015;15(10):1183-1192.
- [CrossRef] [Google Scholar]
- Herd Immunity. Published 2016 (accessed )
- The global polio eradication initiative: lessons learned and prospects for success. Vaccine. 2011;29(suppl 4):D80-D85.
- [CrossRef] [Google Scholar]
- 2019. WHO Removes Nigeria from Polio-Endemic List. Geneva: WHO; (accessed )
- Path to polio eradication in India: a major milestone. Indian Pediatr. 2012;49(2):95-98.
- [CrossRef] [Google Scholar]
- Polio in Nigeria: The Race to Eradication. Center for Strategic and International Studies; 2012.
- 2015. Nigerian National Routine Immunization Strategic Plan. National Primary Health Care Development Agency; 2013-2015 (accessed )
- Systematic Reviews: CRD's Guidance for Undertaking Reviews in Health Care 2009
- Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77-101.
- [CrossRef] [Google Scholar]
- University of Leeds, Nuffield Institute for Health, Leeds. HCPRDU Evaluation tool for quantitative studies. Published 2002 (accessed )
- [Google Scholar]
- Systematic Review Checklist. Published 2013 (accessed )
- The eradication of polio— progress and challenges. N EnglJ Med. 2006;355(24):2508-2511.
- [CrossRef] [Google Scholar]
- Polio in Nigeria: a review of the situation and problems hindering its elimination. Hum Vaccin Immunother. 2016;12(3):658-653.
- [CrossRef] [Google Scholar]
- What is vaccine- derived polio?. Published 2015 (accessed )
- Characteristics of persons refusing oral polio vaccine during immunization plus days - Sokoto, Nigeria 2011. Pan Afr Med J. 2014;18(suppl 1):10.
- [CrossRef] [Google Scholar]
- Progress toward poliomyelitis eradication in Nigeria. J Infect Dis. 2014;210(suppl 1):S40-S49.
- [CrossRef] [Google Scholar]
- An evaluation of polio supplemental immunization activities in Kano, Katsina, and Zamfara States, Nigeria: lessons in progress. J Infect Dis. 2014;210(suppl 1):S91-S97.
- [CrossRef] [Google Scholar]
- An assessment of the reasons for oral poliovirus vaccine refusals in northern Nigeria. J Infect Dis. 2014;210(suppl l):S125-S130.
- [CrossRef] [Google Scholar]
- Cross-sectional serologic assessment of immunity to poliovirus infection in high-risk areas of northern India. J. Infect Dis. 2014;210(suppl 1):S243-S251.
- [CrossRef] [Google Scholar]
- Assessing population immunity in a persistently high-risk area for wild polio virus transmission in India: a serological study in Morabad, western Uttar Pradesh. J Infect Dis. 2014;210(suppl 1):S225-S233.
- [CrossRef] [Google Scholar]
- The Hawthorne Effect: a randomized controlled trial. BMC Med Res Methodol. 2007;7:30.
- [CrossRef] [Google Scholar]
- Performance and determinants of routine immunization coverage within the context of intensive polio eradication activities in Uttar Pradesh, India: Social Mobilization Network (SM Net) and Core Group Polio Project (CGPP) BMC Int Health Hum Rights. 2013;13:25.
- [CrossRef] [Google Scholar]
- Successful polio eradication in Uttar Pradesh, India: the pivotal contribution of the Social Mobilization Network, an NGO/UNICEF collaboration. Glob Health Sci Pract. 2013;l(1):68-83.
- [CrossRef] [Google Scholar]
- Outbreak of vaccine-preventable diseases in Muslim majority countries. J Infect Public Health. 2018;11(2):153-155.
- [CrossRef] [Google Scholar]
- Vaccination greatly reduces disease, disability, death and inequity worldwide. Bull World Health Organ. 2008;86(2):140-146.
- [CrossRef] [Google Scholar]



