

Translate this page into:
Racial/Ethnic Disparities in Preeclampsia, Eclampsia, and HELLP Syndrome Hospitalizations Rates in the United States
✉Corresponding author email: deepa.dongarwar@bcm.edu
Abstract
There is a lack of recent data demonstrating how racial/ethnic disparities in the occurrence of preeclampsia, eclampsia, and hemolysis, elevated liver enzymes, low platelet count (HELLP) syndrome may translate into hospitalization rates. Therefore, the purpose of this study was to evaluate the disparities in preeclampsia, eclampsia, and HELLP syndrome hospitalizations rates across racial/ethnic patient populations in the United States (US). The Nationwide Inpatient Sample (NIS) datasets 2016-2018 were used for this analysis. Prevalence rates were calculated for each hypertensive disorder of pregnancy – preeclampsia, HELLP syndrome and eclampsia, by race/ethnicity. Survey logistic regression model was utilized to find the association between race/ethnicity and each phenotype of hypertensive disorder of pregnancy. During the study period, there were 499.4, 27.0 and 12.1 per 10,000 hospitalizations with preeclampsia, HELLP syndrome and eclampsia. The hospitalization rates and odds of a diagnosis of preeclampsia and eclampsia were higher in Non-Hispanic (NH)-Black pregnant population when compared with NH-White pregnant population. The hospitalization rate and odds of having a diagnosis of HELLP syndrome were highest in NH-Whites as compared to other racial/ethnic groups.
Keywords
Hypertensive Disorders of Pregnancy
Preeclampsia
Eclampsia
HELLP
Racial/Ethnic Disparity
HCUP NIS

Introduction
Hypertensive-related pregnancy disorders are a major cause of pregnancy complications and adverse maternal-fetal outcomes. Approximately 5% of pregnancies are complicated by preeclampsia.1 Of those pregnancies, eclampsia manifests approximately in 1-16% and severe preeclampsia manifests in about 37%.1 Among pregnancies complicated by severe preeclampsia, hemolysis, elevated liver enzymes, low platelet count (HELLP) syndrome occurs in 10-20%.2 However, there are disparities in the prevalence and severity of preeclampsia and its phenotypes among different racial and ethnic sub-populations.3 Understanding how racial disparities play a role in maternal mortality and morbidity is important in improving the care of pregnant patients across the United States. A study published in 2005 reported that Non-Hispanic (NH) Black patients tend to experience preeclampsia and eclampsia more often and have worse outcomes while NH-White patients experience HELLP syndrome at much higher rates than their counterparts.4
There is a lack of recent data that demonstrates how racial/ethnic disparities in the occurrence of preeclampsia, eclampsia, and HELLP syndrome may translate into hospitalization rates.1-3 Therefore, in this study we evaluate differences in rates and the likelihood of preeclampsia, eclampsia, and HELLP syndrome- related hospitalizations across different racial/ethnic pregnant patient populations in the United States (US).
Methods
We conducted this cross-sectional study using the Nationwide Inpatient Sample (NIS) dataset from 2016-2018. NIS is the largest all-payer inpatient care database in the US, containing information on about 7 million (weighted, 35 million) hospitalizations each year.5 Our study sample included all pregnancy-related hospitalizations. The NIS used the International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) to identify all the diagnoses and procedures related to each hospitalization. The following hypertensive disorders of pregnancy were included: (1) Preeclampsia, identified using ICD-10-CM diagnosis code 014.*; (2) HELLP syndrome, identified using codes 014.2*; and (3) eclampsia, identified using codes O15.*6
The rates of hospitalizations for preeclampsia, HELLP, and eclampsia were calculated among all pregnancy-related hospitalizations in the US by race/ethnicity of the patients. An adjusted survey logistic regression model was used to assess the association between race/ethnicity (exposure) and each of the hypertensive disorders of pregnancy (outcome). Covariates included in the study were age, primary payer, zipcode income quartile, and hospital characteristics such as location, bed size, and urban vs. rural. We used two-tailed hypothesis testing for all statistical analyses, and the type-1 error rate was set at 5%. We utilized R version 3-5-1 (University of Auckland, Auckland, New Zealand) and RStudio Version 1∙1∙5001 (Boston, MA) for performing all statistical analyses. The study was implemented on de-identified publicly available data and therefore, was granted exempt status by the Institutional Review Board at Baylor College of Medicine, Texas, United States.
Results
During the study period covering 2016-2018, there were a total of 12,106,775 pregnancy- related hospitalizations, out of which 604,610 had a diagnosis of preeclampsia; 32,740 had a diagnosis of HELLP syndrome; and 14,640 had a diagnosis of eclampsia, corresponding to a prevalence rate of 499.4, 27.0 and 12.1 per 10,000 hospitalizations, respectively.
As shown in Figure 1, the prevalence of preeclampsia (per 10,000 hospitalizations) in pregnant hospitalized women was higher in NH- Blacks (659.3) and Hispanics (506.0) compared to the other ethnic groups. The prevalence of HELLP syndrome was highest in the NH-White group (28.9) whereas the NH-Black (26.0) and Hispanic (25.8) groups had similar rates of HELLP syndrome-related hospitalization. The prevalence of eclampsia was highest in the NH-Black group (23.8), followed by Hispanics (10.5), NH-White (9.8), and NH-Others (9.4).
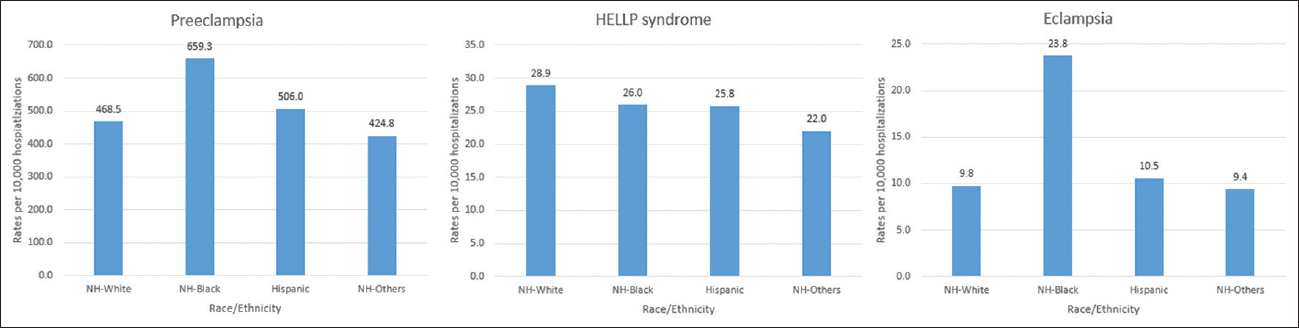
- Hospitalization rates of hypertensive disorders of pregnancy by race/ethnicity
Table 1 shows the adjusted estimates for the association between race/ethnicity and each of the hypertensive disorders of pregnancy. For preeclampsia, we observed increased odds among NH-Blacks (Odds Ratio (OR)=1.34) and Hispanics (OR=1.05), when compared with NH-Whites (referent group). The odds of having a HELLP syndrome diagnosis was highest among NH-Whites, whereas the odds of having eclampsia was 95% higher among NH-Blacks (OR= 1.95, 95% 0=1.77-2.15) when compared with NH-Whites.
| Preeclampsia | HELLP syndrome | Eclampsia | |
|---|---|---|---|
| OR (95% CI) | OR (95% CI) | OR (95% CI) | |
| NH-White | reference | reference | reference |
| NH-Black | 1.34(1.31-1.37)* | 0.98(0.91-1.06) | 1.95(1.77-2.15)* |
| Hispanic | 1.05(1.02-1.08)* | 0.92(0.86-0.99)* | 0.94(0.84-1.06) |
| NH-Others | 0.90(0.87-0.93)* | 0.73(0.66-0.79)* | 0.98(0.85-1.13) |
*Represents statistically significant findings; NH- Non-Hispanic
Discussion, Conclusion, and Implications for Translation
Using the 2016-2018 Nationwide Inpatient Sample database, our study shows that NH-Black patients with preeclampsia and eclampsia had the highest rates and odds of hospitalization. As for HELLP syndrome, we observed that NH-Whites had higher rates and odds of hospitalization compared to all other racial/ethnic patient populations in our study. These findings coincide with prior studies in the literature regarding hypertensive disorders of pregnancy.3,4
Possible genetic involvement may potentially explain the development of HELLP syndrome and other pregnancy-related complications, yet findings on specific genes or inheritance modes for preeclampsia are still inconclusive.7 The hospitalization rates and likelihood observed for preeclampsia, eclampsia, and HELLP syndrome seem to correlate well with what would be expected based on the prevalence of each pathology among different racial/ethnic groups.
The strengths of our study include the large sample size of over 12 million pregnancy-related hospitalizations and the ability to generalize the findings to the US population. As with any national database, potential intrinsic limitations within the NIS, such as coding errors resulting from the usage of ICD codes may have impacted our study findings.
Potential implications for translation from this study include strengthening the literature surrounding the occurrence of different types of hypertensive disorders of pregnancy such as preeclampsia, eclampsia, and HELLP syndrome in different racial/ethnic patient populations. Along with this, our study may assist healthcare providers in identifying high-risk groups for preeclampsia, eclampsia, and HELLP syndrome and for policymakers to implement targeted interventions towards this population. Future studies should explore the root causes of racial/ethnic disparities in hypertensive disorders of pregnancy through the pathway of genetic/biologic determinants, as well as environmental markers.
Compliance with Ethical Standards
Conflicts of Interest:
None.
Financial Disclosure:
None.
Ethics Approval:
None as the study was performed on publicly available data
Disclaimer:
None
Acknowledgments:
None.
Funding/Support:
Research funding support was provided by the US Department of Health and Human Services and Health Resources and Services Administration for Baylor College of Medicine Center of Excellence in Health Equity, Training, and Research (Grant No: D34HP31024).
References
- Delivery Hospitalizations Involving Preeclampsia and Eclampsia, 2005-2014: Statistical Brief #222. In:. In: Healthcare Cost and Utilization Project (HCUP) Statistical Briefs. Rockville (MD): Agency for Healthcare Research and Quality (US); 2017.
- [Google Scholar]
- Preeclampsia: a renal perspective. Kidney Int. 2005;67(6):2101-2113.
- [CrossRef] [PubMed] [Google Scholar]
- Preeclampsia outcomes at delivery and race. J Matern Fetal Neonatal Med. 2020;33(21):3619-3626.
- [CrossRef] [PubMed] [Google Scholar]
- Does maternal race or ethnicity affect the expression of severe preeclampsia? Am J Obstet Gynecol. 2005;193(3 Pt 2):973-978.
- [CrossRef] [PubMed] [Google Scholar]
- Healthcare Cost and Utilization Project (HCUP). Agency for Healthcare Research and Quality. 2012.
- [Google Scholar]
- ICD 10 data. Published October 1, 2021 (accessed )
- Molecular genetics of preeclampsia and HELLP syndrome - a review. Biochim Biophys Acta. 2012;1822(12):1960-1969.
- [CrossRef] [PubMed] [Google Scholar]



